
Indoor Training Questions
Today I want to focus on two practical questions from readers. The first question comes from Bob Fix who is a late 30 something IT person in the Twin Cities.
My question is for those (like me) who want to achieve a higher level of training in the coming year, but are conscious of calories and want to lose more weight: What is the physiological response to “under” nutrition (not enough calories) and more intensive training?
A bit more information, Bob is an avid cyclist and last summer he rode almost 4,000 miles and lost about 20 pounds doing a lot of group rides. He is currently doing about 3-4 indoor aerobic workouts of around an hour per week and strength training 1-2 times per week. The aerobic workouts include some higher intensity efforts. Bob also wants to avoid gaining weight this winter so he is ready to go when it warms up. He is currently counting calories and really watching what he eats and shooting for about 1900 calories per day. Here is a summary of some ideas I shared with Bob:
- For bang for the buck indoor training I prefer the type of interval workouts I have outlined in the blog. This approach keeps you cardiovascular fitness high and then when Spring/Summer rolls around you are good to go. It looks like the workouts you sent have some of these elements so if they are working, keep doing them. Weights a couple of times per week are also a good idea as will be discussed in a bit more detail in response to question #2 below. So, I think you have the bases covered in terms of winter working out.
- Biking on the road is always essentially interval or fartlek training due to hills, drafting, the wind etc. So this is another reason to do some higher intensity exercise during your indoor sessions this winter.
- About counting calories, see what the 1900 cals/day does to your working out. If you feel overly “wasted” and are not recovering then up the calories a bit. The other issue in the winter is the temptation to drink a bunch of beers and eat a plate of wings or something while watching a football game. To avoid situations like this, people who are successful at keeping weight off typically have plenty of carrots and low calorie snacks around to munch on. There is also at least some evidence that people who work out for longer overestimate the calories they are burning, or that more prolonged exercise stimulates their appetite and can make it harder to keep weight off. When you are doing multiple hours of riding per day in the summer this is likely less of an issue, so calorie counting can be important for people when they are doing the types of workouts you describe.
Summary, see how the diet goes and make minor adjustments so that your training does not suffer. More weight will come off when you get outside and the duration of your weekly training picks up. The key is to not lose what you gained in terms of fitness and to gain what you lost in terms of weight over the winter.
The second question comes from Dr. John Schmidt a colleague who is a research and clinical psychologist at the U of Pittsburgh.
I would be very interested in your thoughts on weight training worked into a typical fitness routine. I recall much controversy regarding the use of weights and the potential for detrimental vascular effects.
Here are a few thoughts on this topic:
- Current guidelines now emphasize the need for strength training for middle aged and older adults. The concerns you mention have not panned out and a bigger problem is that many middle aged and older people lack the strength to do their activities of daily living. Grip strength is also a powerful predictor of health as we get older, and it is even predictive in younger people.
- There is some controversy for more competitive people about whether cyclists or runner for example should do weight training with their legs. For cycling some studies are positive and others are negative so there is not clear answer and there is also no clear answer for running. However, there are some positive indicators in more elite runners. For both cycling and running it is probably a matter of whether the fatigue associated with the strength training interferes with the quality of the cycling or running training. Things might also be different for recreational participants vs. more elite athletes.
Summary, resistance training is a key component to overall fitness and health. The winter might be a good time to experiment and see what works for you. This is especially true for more competitive people who want to see if strength training their legs will improve their cycling or running.
In answer to both questions I would urge people to use the cold months to experiment and see what works for them. This will keep you mentally fresh and provide you with some new ideas for when warms up.

Bait & Switch: Longevity and the Medicare Eligibility Age
In a post last week I reviewed data on life expectancy and implications for the retirement age especially in the context of proposed changes in the eligibility of Medicare. Here is a link to a retirement age calculator for the U.S. Social Security system. For those born after 1938 the age gradually increases to 67 for those born in 1959. The retirement age for Medicare is currently 65, but up for discussion in the ongoing debates about the fiscal future of the U.S.
The idea driving the Medicare debate is that people are living far longer than they were when the program was started and thus an upward adjustment is needed to make Medicare demographically realistic and limit the explosive (and unsustainable) increases in costs for this program as the baby boomers retire. Opponents of this idea point out gains in life expectancy have been uneven and that most of the gains have been in relatively well-off segments of the population. There are also significant life expectancy differences based on race, education and sex (women live longer). Thus, the idea is that raising the retirement age would be “unfair” to certain groups. As I pointed out last time, no one ever brings up the general “unfairness” of these programs to men which I find a bit puzzling but will leave to the pundits to sort out.
The counter argument about the potential unfairness of raising the eligibility age for Medicare is that the real problem is what happens to or in the groups with lower life expectancy before age 65. In other words, the differences in life expectancy in various subgroups for those who make it to 65 or older in pretty good health are less dramatic than the differences in life expectancy from birth data would suggest. What follows are some examples of what happens to people before age 65 that might explain some of the socioeconomic differences in life expectancy.
Physical Activity
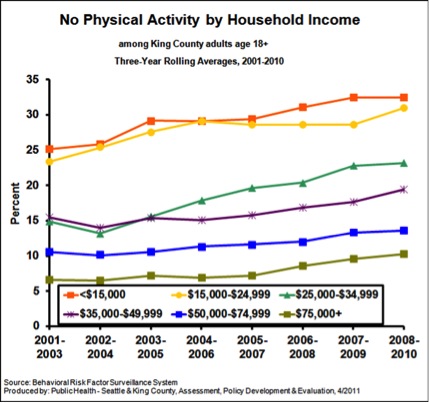
The figure below is from King County, Washington (Seattle) and shows data on the influence of income on “no physical activity in the last month”. As I have pointed out repeatedly, physical activity is extremely protective against all sorts of problems and increases longevity dramatically.
Obesity
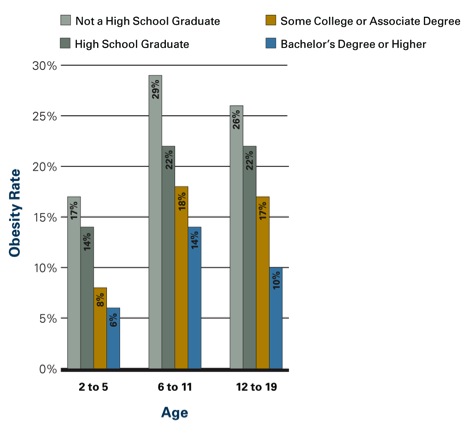
The figure below shows the influence of parental education on obesity rates in kids. Similar data is available for adults. In adult women those with more education and higher incomes are less likely to be obese. In men the relationship is not as clear, but there is some evidence that better educated men are less obese the less educated men. However, the bad news is that obesity has increased for both sexes and all socioeconomic and racial subgroups in the last 20 plus years.
Smoking
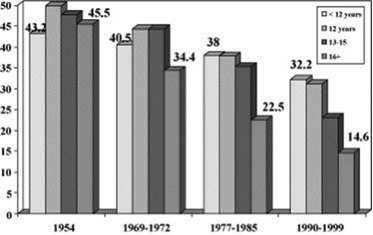
The figure below shows data on smoking rates by education (usually a close correlate of income) and how they have changed between 1954 and the 1990s. Rates have fallen for all groups but most dramatically for the most educated people.
Social Stress
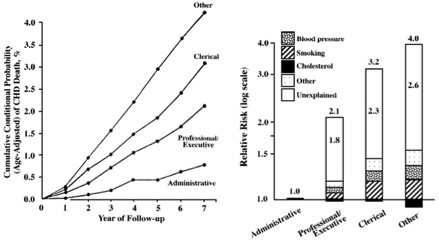
There is pretty good evidence that social status and what might be described as social stress and autonomy plays a role in the early mortality seen in less educated and lower socioeconomic status groups. In other words, poor and less educated people have less control over their daily lives and that is stressful and bad for their health. Social stress is also independent of traditional risk factors or access to care. The figure below shows how job category/education affects cardiovascular mortality in civil servants in England. The bar graph on the right of the figure is a “log-scale” so a bit distorted, but the overall picture is clear. The article points out that:
The cardiovascular mortality rate over 7 years in 17 530 London civil servants was more than 4% among unskilled workers, compared with 3% among clerical workers, 2% among professionals or executives, and less than 1% among administrators. The presence of identified risk factors, including cholesterol level, blood pressure, and smoking, explained less than half of these differences. All of these persons were working at the onset of the observation period and had access to medical care through the National Health Service. Therefore, neither biomedical risk factors nor limited access to medical care can account for most of the differences, and the major component of differences in the risk for cardiovascular death remains. We suggest an explanation based on lifestyle and behavioral considerations.
My bet is that the more educated and higher paid civil servants in the UK were much more likely to be physically active, watch their diets and otherwise comply with health guidelines and medical advice.
Summary
All sorts of issues including physical inactivity, obesity, smoking and social status/stress need to be addressed to reduce the effects of socioeconomic status, education and race on life expectancy. However, most or all of these issues need to be addressed prior to the age of 65 to have much of an effect on life expectancy. Most are also relatively independent of access to medical care. Confusing these issues, with the eligibility age for and long term finances of Medicare is an example of a policy discussion bait and switch.
BMI, Mortality & Health
There was a lot of attention in the press last week about a new report in the Journal of the American Medical Association (JAMA) showing that BMIs in the “overweight” category (25-30) are associated with lower overall mortality rates. This was accompanied by editorial comments about the need for people to calm down about the fact that U.S. in specific and the world in general is getting fatter. Before taking a deeper dive into the BMI vs. mortality argument here is a link to a post on BMI, and recent overweight/obesity trends in the U.S.
What is the relationship between BMI and mortality?
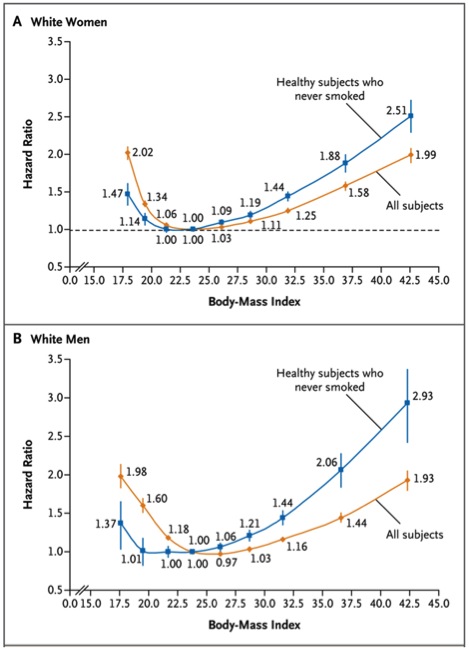
The figure below is from a study of almost 1.5 million whites between the ages of 19 and 84 with a median age of 58. This study has a couple of advantages over the JAMA study especially because it was prospective as opposed to a meta-analysis of prior studies. However, it is restricted to only one racial group. The study also shows that the relationship between mortality and BMI does not really “take off” until people get into the obese (BMI > 30) range. However it is not as reassuring as the JAMA study and mortality does start to creep up in the overweight (BMI 25-30) range. The study concludes that:
“In this large, pooled analysis of prospective studies, both overweight and obesity (and possibly underweight) were associated with increased all-cause mortality in analyses restricted to participants who never smoked and did not have diagnosed cancer or heart disease. Thus, analyses of this subgroup should be minimally confounded by smoking or prevalent illness. The associations were strongest among participants whose BMI was ascertained before the age of 50 years. The lowest all-cause mortality was generally observed in the BMI range of 20.0 to 24.9. Longer follow-up attenuated the associations with lower BMI levels.”
BMI Caveats
The small increases in mortality for the overweight and mildly obese are somewhat reassuring; but the whole relationship between BMI and health is tricky. There are high BMI people who have a lot of muscle mass and not much body fat, and there are low BMI people with a lot of fat who have poor health and increased mortality. This has been termed normal weight obesity, and suggests that low muscle mass can also be a problem. Low muscle mass might also explain some of the mortality issues in people with very low BMIs (<20). There are also high BMI people with plenty of body fat who have normal cholesterol and glucose who are “metabolically healthy”. Thus, there are several patterns of body composition and BMI does is not that predictive on an individual basis. In general abdominal obesity tends to be a bigger problem than fat other places. Here is a link to a Wiki site on abdominal obesity that is informative. Finally, exercise can also modify the relationships between BMI and metabolic health in people in the overweight and obese categories. This is the whole “fit vs. fat debate”.
Mortality vs. Health?
The BMI mortality data does not tell us much about overweight/obesity and health, and this data is hard to come by. However, there is good evidence that so-called biomarkers of disease risk show a more linear vs. U-shaped relationship between BMI and the marker of interest than between BMI and mortality. The figure below shows this for men with data from a large national survey. CRP is a marker of inflammation related to heart disease risk, HBA1c is a marker related to diabetes, and HDL is so-called “good” cholesterol. The panels on the left were statistically adjusted for age and the panels on the right for age and smoking. In the long run the increased risk factors associated with higher BMIs will likely translate into poorer overall health for many people. The authors conclude that:
”These findings imply that obesity researchers should exercise caution when interpreting mortality findings in broader health terms. From a public health perspective, the findings suggest that even moderate levels of overweight may indicate worse health risk profiles than lower body weights, with potentially important implications for chronic disease and health-related quality of life……”

Summary
The relationships between BMI, mortality and health are complicated. Based on the data above we probably should take the “don’t worry” interpretation of the findings in the JAMA paper promoted in the mass media with more than a grain of salt. We also need to think about overweight and obesity using more sophisticated measures of body composition, and a one size fits all BMI based approach to these issues leaves a lot to be desired. The data from the “normal weight obese” and “fit vs. fat” studies along with the very low BMI subgroups in the big population studies suggest that the role of active muscle mass in our overall health is underappreciated. Finally, people tend to gain weight over the years and many of the overweight of today are likely to be the obese of tomorrow.
Lance: He’s Back?
There are news reports that Lance Armstrong is considering coming clean and admitting that he doped. Back in October I speculated that this might happen, and at least some of this may be about his desire to compete in high level triathlons. As I think more about it, the average observer may not be fully aware that a subset of super-elite athletes really “needs” the combination of fame, glory, money, and adrenaline that comes from being at the absolute competitive edge. My bet is that Lance is thinking that with a suspension lasting between 2-4 years he would be back by his middle 40s with just enough “physiological time” left to win the Ironman. It would be a stretch, but some folks in their early 40s have done very well at that distance and it is certainly not physiologically impossible. If Lance did it, he would get everything he seems to crave…… at least for a while.
Longevity and the Retirement Age
Much of the long term pressure on the finances of the Federal Government is being driven by rising expenditures on health care and pensions and much of this is being driven in turn by an aging population. This has led to proposals to raise the retirement age especially for Medicare. You will likely be hearing more about the retirement age as our political “leaders” try to figure out what to do next in terms of taxes and spending.
Here is a proposal from the conservative Heritage Foundation on this topic, but they are not alone and many “centrist” groups are proposing increases in the retirement age for Medicare. This idea has been criticized by people like the economist turned political commentator Paul Krugman as unfair because the increases in overall longevity in the U.S. have been uneven and not shared by all socioeconomic and racial subgroups in the country. Today I want to take a deeper data driven dive into this topic.
1. The big picture. In an earlier post on longevity I pointed out that in 1960 about 60% of men and 71% of women lived to age 65. The men who made it to 65 then lived an average of about 13 years and the women who made it to 65 lived another 17 years. In 2010 about 84% of men and 89% of women made it to 65. The average man who makes it to 65 now lives another 16-17 years and for women it is about 19 years. These changes are being amplified by the fact that the leading edge of the baby boom generation is reaching retirement age causing a further bulge in the aging population. You don’t have to be a rocket scientist to realize these demographic trends are putting pressure on Federal finances.
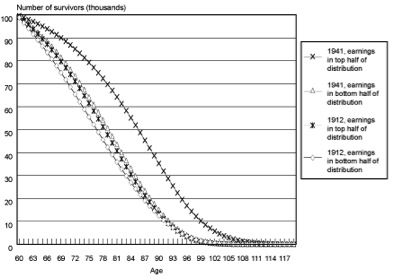
2. Differential Increases in Longevity and Socioeconomic Status. I mentioned above that critics of the idea of raising the retirement age for Medicare point out that most of the gains in longevity have been in people that are relatively well off. The graph below is from a study by the Social Security Administration and shows survival curves starting at age 60 for men comparing those born in 1912 with those born in the 1941. The key observations are that: a)in 1912 there was not much difference in life expectancy between the top and bottom half of income distribution, b) the bottom half of the 1941 cohort does not look that different than either group from 1912, and c) that life expectancy at age 60 has really gone up for the better off men born in 1941. There are lots of ways to slice and dice data like this but pretty much every way you do it comes out the same and gains in life expectancy have been greater for people who are better off.
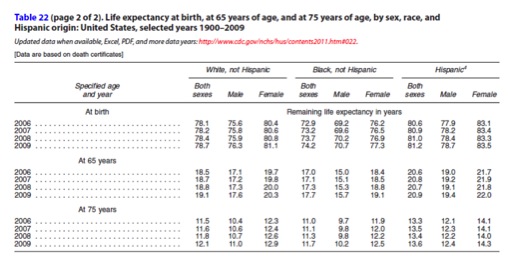
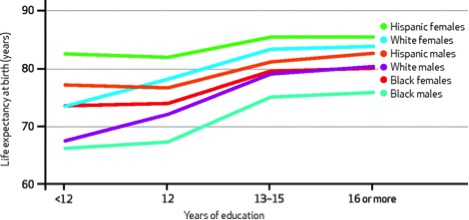
3) The race and education snapshot. Below are a table and graph from summary data from the U.S. Centers for Disease Control in 2011. The table shows life expectancy at birth, 65, and 75 in recent years. What is interesting here is that the differences in life expectancy between Blacks and Whites at 65 and especially 75 are much lower than the projected differences at birth. The other interesting thing to note is that Hispanics are higher than either Blacks or Whites in all of the major comparisons. I interpret this in a couple of ways. First, a big issue here is not what happens once people reach the standard retirement age of 65, but what is happening prior to age 65 especially in Blacks. The other issue here is that women do better than men and I have not heard any of commentators claim that raising the retirement is unfair to men.
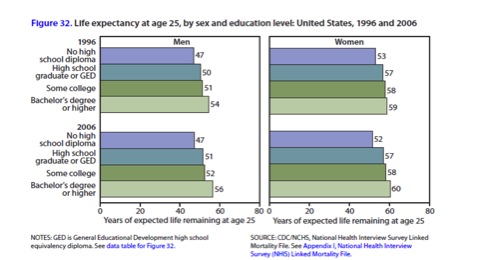
The next figure shows life expectancy at age 25 in 1996 and 2006 by education level and sex. This table shows a couple of things including: a) educated people live longer and there is a dose response curve, and b) life expectancy at age 25 for less educated people has stagnated. This figure also shows that women live longer than men at every level of education.
4) A summary slide. The figure below is a summary slide that shows the effects of race, sex, and education on life expectancy at birth. These differences would likely exist at age 65 but be much smaller in terms of absolute years. The article this figure was taken from indicates that some of these differences might be getting worse.
My take on all of this data. There are all sorts of ways this data can be analyzed. For the purposes of thinking about the retirement age a couple of things stand out.
- People as a whole are living longer but the gains have been uneven and influenced by sex, education, and race. There are also probably pretty tight relationships between race, economic well-being and education.
- A lot of the problem is not about what happens when people reach age 65, but what happens before age 65. People with lower socioeconomic status tend to have a host of behavior and risk factor issues that negatively influence their ability to make it to 65 and then do as well after age 65. So the real issue here is how to address health disparities vs. the fairness of raising the retirement age.
- Many of the factors leading to health disparities like differential smoking rates, obesity, lack of physical activity, and violence have little to do with what we think of as traditional health care and will not be fixed if and when high quality health care is available to all.
- There is also an argument that people are retiring too early for economic reasons and that a lot of people are financially unprepared for the long life they are likely to live in retirement. If raising the eligibility age for Medicare encourages people to work longer, maybe that is good for their own long term economic well-being as well as that of the country as a whole.
Closing comments. The discussion about the fairness of raising the retirement age for Medicare has been marked by incomplete thinking about the data and is confusing the very real problem of what to do about health disparities based on race, education, and sex with the arithmetic of Federal finances. Some of this discussion is being led by people with overtly political and personal agendas like Paul Krugman (who should know better) at the expense of a hard look at the facts.
Mastery for New Years?
In the Thanksgiving and Christmas posts I focused on optimism and mindfulness. For New Years I want to focus on the complementary concept of mastery. Together they operate like a “three legged stool” and can provide a balanced approach to almost any challenge.
Benny Goodman (1909-1986) was one of the all-time great clarinet players. He was also a leader in the emergence of jazz as a respected and mainstream art form. Beyond that he integrated his band in the 1930s more than 10 years before institutions like professional baseball or the U.S. military were integrated. Underneath all of this innovation and personal excellence was an obsessive devotion to practicing the fundamentals of the clarinet. In fact, during the 1950s at the height of his fame, Goodman started taking lessons again to improve elements of his playing so he could master classical music as well as jazz. How many of us who are really skilled and famous at something would seek out a teacher or coach to branch out and get better in middle age? One overriding lesson in all of this is that Goodman’s mastery of and focus on the basics served as a platform for him to break new ground and take chances in multiple arenas.
The clip below shows Goodman and his band playing “Sing, Sing, Sing” in the late 1930s as part of the movie “Hollywood Hotel”. Note how relaxed he and the band are. Note that he lets the great drummer Gene Krupa and trumpet player Harry James get plenty of attention. At the end of the clip he is playing with the equally gifted Lionel Hampton and Teddy Wilson who were black which would have been inconceivable pre-Goodman.
click here for video
Are there larger lessons from Benny Goodman? It seems to me that we have entered into a world of mindless standardization and metrics that inhibit change in the name of stability and predictability. Our ability to measure all sorts of things that might be called outcomes and then manage the world in an effort to get more of the “desired” outcomes in a sort of linear way has never been greater. However, life is unpredictable and perhaps what is missing in all of these metrics is the recognition that improvisation and novel solutions are what move our messy world forward. So, do we mindlessly focus on metrics or do we use metrics as a way to ensure we have mastered the fundamentals of whatever we are doing? We can then use our mastery as a platform to innovate and take chances like Goodman did.
Perhaps the best example of metrics gone bad comes from the Vietnam War when things like body counts were used by Secretary of Defense Robert McNamara as a substitute for insight about the nature of the war. If you want to see a chilling example of a leader who does not understand the importance of culture and the non-rational elements of life, the documentary film “Fog of War” by Errol Morris is an extended interview with McNamara at the end of his life. He went to his grave not getting it and thinking that everything could be subject to metric driven analysis and decision making.
On the flip side is the W.L. Gore Company that makes Gore-Tex and other interesting products. Gore has rejected the top-down metric driven world view and things like economies of scale. Instead they focus on a few key values and trust their employees to move the company forward. They keep their work units small (less than 200 people) and intimate on purpose. One size rarely fits all and this idea is now getting more play by the people who study long term organizational success. Mindless adoption of best practices merely accelerates the arrival organizational monocultures and dogma that limit our ability to adapt to rapidly changing circumstances. In medicine many of the key guidelines and best practices I learned in the 1980s and 90s have been turned on their head. Best practices are only best for now.
What would Benny say? The clip below is from an interview Goodman did late in life with Diane Sawyer……my take on what he said is that it is all about mastering the fundamentals to do unique and challenging things. Being a slave to metrics and standardization are easy and tempting ways to limit your ability or the ability of your organization to move forward. The next time you hear someone tell you they are managing to metrics, ask them what they might be missing!
click here for video
Indoor Exercise: Tips for the New Year!
This is the time of year where people in colder climates do more indoor exercise. People also make New Year’s resolutions to get in shape. Some serious athletes use indoor training year round because it is possible to better control the exercise intensity and the overall effort of the training session on a treadmill or bicycle ergometer. All of this is easier now than it was 20-30 years ago before the widespread availability of well-equipped fitness centers.
However, indoor exercise can be boring and it is easy to lose fitness this time of the year. Getting to the gym can be a hassle and short days along with the urge to sort of hibernate during the winter can make finding time to train a bit harder. So the question is how to get the most bang for your training buck until it gets warmer and the days get longer?
One thing I do is interval train on the Treadmill 2-3 times per week. I start slowly about 6.1 miles per hour (mph) and then use a saw tooth pattern of increasing speed. I go up 0.5 mph on the even numbered minutes and down 0.2 mph on the odd numbered minutes. After about 10 minutes I get to a pace of around 7.7 mph and then do 10 repeats of 1 min at 7.7 mph followed by two minutes of running in the 8.5-9.5 mph range. The goal is for each of the two minute repeats to be at a faster speed. In interval training lingo that is known as “descending” the workout. A Lot of times I increase my pace by 0.1 mph every 10 breaths, so I pick it up during the fast part of the cycle. Counting your breaths is also a good way to learn to relax while you are running fast. Using this pattern, the first mile is almost exactly 9 minutes and then I try to do a bit over 4 miles in the next 31 minutes. The total session takes 40 minutes.
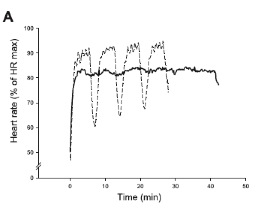
Along these lines there is an excellent recent paper from colleagues in Denmark on the efficacy and efficiency of this type of training strategy. They asked moderately fit people in their 30s who had been running about 15-20 miles per week to either keep doing more or less the same thing or do three sessions a week of interval training for seven weeks. The intervals consisted of three or four 5 minute intervals with two minutes of jogging in between. However, during the fast part of the intervals low-, moderate-, and high-speed running (<30%, <60%, and >90% of max) for 30, 20, and 10 seconds was used each minute. This is pretty complicated to describe but the figure below shows a typical heart rate pattern for such a training session. The heart rate shown with dashed lines is higher during 5 minute intervals and lower during the recovery period than during a steady state training session shown with the solid line. The slight variations in heart rate during the intervals are due to the 30-20-10 changes in running speed.
Key findings included:
- The interval training group reduced training volume by 54% (14 vs. 30 km/wk about 9 vs 18 miles/wk) while CON continued the normal training.
- After seven weeks VO2max (a key marker of fitness), and performance in a 1,500-m and a 5-km run improved by 21 and 48 s, respectively.
- Blood pressure and cholesterol values also improved more in the interval training group.
The authors concluded that:
“The present study shows that interval training with short 10-s near-maximal bouts can improve performance and V̇O2max despite a ∼50% reduction in training volume. In addition, the interval training regime lowers resting systolic blood pressure and blood cholesterol, suggesting a beneficial effect on the health profile of already trained individuals.”
Summary
Relatively brief but high intensity interval training is a great way to maintain and even improve your fitness in the winter. For people with competitive goals it means that you will be ready for more and harder training as the days get longer and warmer and you head outside in March or April. There is also a growing body data about the value of higher intensity exercise for people of every ability level and age group. A New Year’s resolution that includes interval training might be a good way to start.
Mindfulness for Christmas?
In my post around Thanksgiving I made the case for optimism as a justifiable approach to the world. The general idea is that many things have gotten better and many seemingly unsolvable problems have been addressed in the last 40 or so years. Part or my motivation was reminding people that life goes on and things frequently get better no matter how crazy the world seems at any given moment. In the past few weeks a number of things have led me to think that optimism and something called mindfulness go hand in hand.
First, what is mindfulness? One way to look at it is just simply paying attention or being more engaged in what you are actually doing. In other words stop distracting yourself. Tough to do in a world full of electronic and other goodies and interruptions. Based on personal experience and chatting with others, I think a major reason people who are committed exercisers stay with it is because their exercise time is something they “own” and includes a chance to focus and get into what is usually called the “zone”. The elite athletes do it and so can you. When it happens you too can be a religious mystic………
Below is a little brain candy about mindfulness that you can give yourself for Christmas:
- Here is a link to an interesting article on mindfulness and the need to sometimes let things percolate. There is a saying in medicine “don’t just do something stand there!” Wise advice to consider before you push the overreact button, or respond too quickly to an irritating e-mail. There is no retrieve button, and part of life is learning what to ignore.
- The book ”Finding Flow” has a number of ideas about how to get more “Flow” into your life. From what I can tell flow, mindfulness and the zone are different names for the same thing. A quick summary might be the internal satisfaction associated with engagement in a challenging activity and doing it well for its own sake independent of an external outcome. Not too different from the definition of success and other ideas promulgated by legendary basketball coach John Wooden. Wooden learned in his early 50s that shorter practices devoted almost exclusively to a limited number of fundamentals and simple plays paradoxically made his teams better. At the same time he stopped scouting the other team preferring instead to devote his energy (and the energy of his team) to what they had total control over…….their focus, effort and execution. Coach Wooden had learned to ignore or maybe how to focus by ignoring.
- There are some good resources about how to use what might be called micro breaks to do a little deep breathing and refocus throughout the day. My colleague and collaborator John Schmidt, a psychologist at the University of Pittsburgh, has used these techniques to help people with chronic pain move forward and get more out of life. John tells me they can work for us all and he recommends the short book “Wherever You Go, There You Are”. Here is a handout he uses with his patients.
- In some of my posts around the Olympics I highlighted what the great coaches know and how they help the athletes they supervise “relax and win”. In other words put forth seemingly super human efforts effortlessly. These very same approaches can help us all.
- My friend Terry Laughlin, who is one of the great coaches, has two interesting recent posts on his blog. One is related to mindfulness, adult learning and successful aging. Terry started off many years ago trying to help people swim faster and now he helps them understand that the fastest swimmers swim slower (fewer strokes to cross the pool) using less force. His second post is about how a video of one of his disciples became the most watched swimming video ever. In e-mail conversations with Terry he has taught me that to streamline your swimming stroke you must first streamline your mind (just like Coach Wooden streamlined his approach). Perhaps there is a more general principle here to streamline your life……your organization……your whatever, perhaps you must first streamline your own mind.
So maybe give yourself the gift of mindfulness this Christmas. And remember the words of Antoine de Saint-Exupéry who wrote the “Little Prince” and was also a pioneering aviator. His advice below might seem counter-intuitive, but less truly is frequently more and the examples highlighted above are just a few that prove the point. Enjoy the process of streamlining your mind in 2013.
“…perfection is finally attained not when there is no longer anything to add, but when there is no longer anything to take away…”
LIKE MIKE

SUBSCRIBE TO RSS
