
Obesity vs Fast Food Availability
Most people who read this blog probably don’t have to be convinced about the link between eating a lot of fast food and obesity. However, I wanted to find out just how big the link is and see what else I could learn about this relationship. Here are some interesting findings.
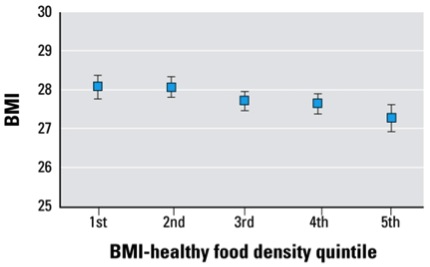
BMI vs. Healthy Food Outlets in NYC.
The figure below is from a study in New York City on the density of healthy eating options vs. BMI. It tracked about 13,000 people and rated the density and quality of food outlets (supermarkets vs. fast food etc.) in their neighborhoods, rated them, and then divided the food ecology into quintiles (fifths). The study also corrected for things like neighborhood walkability and other factors known to influence body weight in the population. A person of average height living in the healthiest food neighborhoods (5th quintile) would weigh about 5-8 pounds less than a person living in the worst neighborhoods (1st quintile). Depending on your perspective, that might not seem like a lot but either losing or gaining just a few pounds can have marked effects on things like your blood sugar and blood pressure.
What about LA?
Los Angeles is very different than New York City. This is especially true in terms of dependence on cars and the presence or absence of convenient public transportation. So, what is the relationship between fast food restaurant density, driving and body weight in LA?
“ Car owners have higher BMIs than non-car owners; however, individuals who do not own cars and reside in areas with a high concentration of fast food outlets have higher BMIs than non-car owners who live in areas with no fast food outlets, approximately 12 lb more (p = 0.02) for an individual with a height of 5 ft. 5 in. Higher restaurant density is associated with higher BMI among local residents. The local fast food environment has a stronger association with BMI for local residents who do not have access to cars.”
Driving and Fast Food Signs.
As noted above car owners in LA have higher BMIs than non-car owners. The obvious explanation for this is that they are less physically active and that sitting in a car contributes to weight gain over time. However, we all see road signs while driving. Does the presence or absence of road signs influence body weight? A very creative study on this topic found that:
“The higher the percentage of outdoor advertisements promoting food or non-alcoholic beverages within a census tract, the greater the odds of obesity among its residents, controlling for age, race and educational status. For every 10% increase in food advertising, there was a 1.05 (95% CI 1.003 – 1.093, p<0.03) greater odds of being overweight or obese, controlling for other factors. Given these predictions, compared to an individual living in an area with no food ads, those living in areas in which 30% of ads were for food would have a 2.6% increase in the probability of being obese.”
This data adds to all sorts of information showing that “marketing works”. What we see while we drive makes a difference.
What Happens if Fast Food Outlets are Restricted?
The data above provide pretty good evidence that the type of food outlets, driving and advertising influence body weight and are contributing to the obesity epidemic (no big surprises here). However, cities can regulate how many fast food restaurants there are and where they are located via zoning and licensing. If the density of fast food restaurants were reduced what would the impact be? This is especially important because many poor neighborhoods are so-called healthy “food deserts” and obesity is an especially big problem in these areas. The interactions between income, neighborhood walkability, and the type of food outlets are complicated. However, small changes in the local food and walking ecology can make a big difference in obesity statistics and ultimately public health.
Summary
There is a lot of discussion about “soda taxes”, expect to hear more about advertising and efforts to regulate fast food outlets in the coming years as public health efforts to attack the obesity epidemic accelerate.

On The Road Again
I have been doing a lot of traveling in the last month. Some of it has been to great places to be physically active like Ft. Myers Beach, Florida, which has the best beach for running or walking I have ever been on. The beach is very long, and the tide usually comes in high enough to keep a nice flat shoulder of it firm which is perfect for running or walking. You also see plenty of pelicans dive bombing for breakfast and sometimes there are dolphins swimming close to shore.

The other places I have been were business travel. My stop wherever usually includes a stay at a nameless faceless hotel with a reasonably good work out area, but they vary. After a while though there is only so much you can do for so long in a hotel exercise room. Ten years ago when I was mostly swimming for exercise, I would obsessively find a pool to use in almost every city in the world. The “Swimmers Guide” website never failed me. Perhaps the most exotic and beautiful places I have been swimming are the salt water rock pools of Sydney, Australia. If you ever get the chance, go!

However, my obligations during business travel seem to be starting earlier in the morning and going all day. As a result, I am less inclined to go to the logistical headaches of finding a place to swim unless it is really convenient or there is a beautiful outdoor pool like the one in Coronado, California near San Diego in the area. However, while on the road I am careful about how much running I do for injury avoidance reasons and I want to make sure I do plenty of whole body training as well. Additionally, while most hotels have acceptable treadmills, the quality of the exercise bikes is pretty variable. So, what have I been doing?
Circuit Training is the Answer!
While traveling, I run either outside or on the treadmill for 30-40 minutes every other day. If there is a reasonable exercise bike in the hotel sometimes I do 30 minutes of cycling followed by 20-30 minutes of running. I use the timer on my watch to do things like one minute jog, one minute fast to break things up and keep my exercise intensity high. On the alternate days I have been doing cycling or jogging for a few minutes interspersed with whole body calisthenics and weights. Here is a sample circuit work out from a few days ago.
- 5 minutes of easy cycling
- 20 burpees followed by leg-raises/crunches followed by dumbbell curls and rows
- 2 min cycling
- 40 stair climbers followed by planks followed by push-ups.
- 2 min cycling
I then repeated this for 40 minutes of total exercise with 5 minutes of easy cycling for a cool down. When I am outside the cycling is replaced jogging. I also vary the combination of exercises I do and as this type of session goes on I am lucky to be able to do 10-12 burpees or 30 stair climbers. If there is a lat pull machine or a place to do pull ups or bar dips I work those into the routine as well.
So far this has worked well, is convenient and a great way to start your day while on the road. I have noticed that when I get home and into the pool or on the bike I have not lost much and am ready to go right away. This has also been a chance to vary things and be creative. I am thinking about adding jump-roping to the routine in place of the jogging or cycling, and I have seen other folks use medicine balls and sand bags with their calisthenics at some of the better hotel exercise rooms.
Summary: There are plenty of low-tech solutions to the challenge of exercise while on the road or really the challenge of exercise anywhere. Find one that works for you!
Medicare’s 2 for 1 Challenge!
I want to get back to issues associated with Medicare in specific and the demographics of aging in general. Part of the reason for this is that the rate of increase in Medicare spending seems to be slowing a bit and that is leading at least some of our political leaders and commentators to suggest we pay less attention to the long term implications of Medicare spending for the U.S. Federal Budget and economy. That having been said I want to make a few points that we should all be thinking about in terms of our own retirement planning, our kids and also friends and relatives who are older.
Point 1: The number of workers per retiree continues to drift downward.
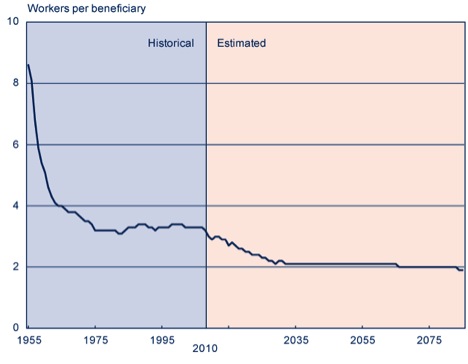
The figure below is from the Social Security Administration and it shows both historical data and future projections for the number of workers per retiree. The magic number here is that over the next 20 years, if nothing changes, this ratio is going to drift downward from about 3.4 to 1 and stabilize at roughly 2 to 1. Medicare (and also Social Security) is ultimately a pay as you go plan. So the question is how much can we expect younger workers to pay to cover benefits for older people? This is especially interesting because for better off older people, we currently have a situation where younger people of modest and limited means are essentially subsidizing a large portion of their health care costs. Is this a wise policy? Is it fair? Is it even ethical?
Point 2: What Happens After the Baby Boomers are Gone?
I did a little thought exercise with my friend and colleague Bob Smoldt, an extremely experienced medical administrator, who has great expertise about all of the economic aspects of health care. I asked Bob what is projected to happen after 2045 when about half of the baby boom generation (born between 1946-1964) will likely be dead. My thinking was that once we are over the demographic hump associated with the baby boom, perhaps the number of beneficiaries would stabilize or drop and the 2 to 1 ratio would get better. Here is an excerpt of his response:
“What happens after baby boomers are gone? Does the problem get better? It is quite interesting. Here is what the latest Medicare Trustees Report (2012) projects:
Number of Medicare beneficiaries
- 2045 = 88.7 million
- 2055 = 93.3 million
- 2065 = 99.8 million
There is no decrease projected. I assume this is at least partly because of expected increase in life expectancy. So if you want to save entitlements by having the Baby Boomers die off — they better do so more quickly……
Ratio of workers (people paying the bill) to beneficiary
- 1970 = 4.6
- 2010 = 3.4
- 2030 = 2.3
- 2085 = 2.1
Workers per beneficiary levels off from 2030 – 2050 and then declines even further to 2.1. I don’t know why Social Security is different, but they project workers per SS beneficiary going down to 1.9. I was a bit surprised by this, but there is no magic bullet here. It just keeps getting worse — we will basically be at 2 workers per beneficiary “
Point 3: Potential Solutions.
It seems to me that these statistics are pretty hard to ignore and that sooner or later Medicare is going to have to be reformed. Here are a couple of ideas about what to do that could be adopted alone or in combination.
- Raise the retirement age. I have discussed this in detail before and challenged the idea that raising the retirement age is unfair to certain ethnic and socioeconomic subsets of the population with lower life expectancies. The issue here is largely who makes it to 65 vs. survival after age 65.
- Means test benefits so that well off people get less. This is an old idea and the link earlier in the post on younger people subsidizing well off older people discusses how this might work and includes adjustments for groups with lower life expectancies.
- The other idea is so-called premium support similar to what members of Congress get. Here is a comparison of several proposed plans. This idea has recently been derided as “VoucherCare” by liberal political commentators even though it was originally proposed by liberal think tanks.
Answers From Scandinavia?
Some conservatives love to make inflammatory comments about how President Obama is trying to turn the U.S. in to Western European style social democracy with a cradle to grave welfare state. I have a different observation; countries like Sweden are in fact reforming their social welfare systems much faster that the U.S. is via things like raising the retirement age and going to defined contribution funding models. The Swedes for all their alleged liberalism seem to be recognizing demographic reality and dealing with it. While Sweden changes the U.S. is trapped in a vicious cycle of demographic denial.
The Beginning of Good News on Obesity?
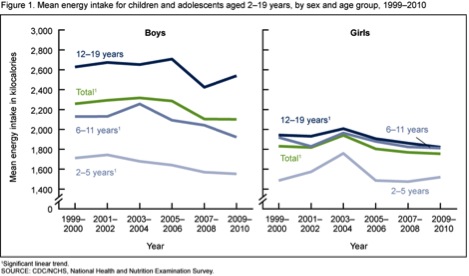
There are two recent reports from the United States Center for Disease Control about obesity and calorie consumption that make me a bit more optimistic that the obesity epidemic might be cresting. The first report shows what looks like the beginning of a decline in calorie consumption by kids over the last 10 years but especially during the last 5 years. The figure below is taken from this report. There are all sorts of caveats about this data but it is promising and seems to correlate with the idea that childhood obesity is leveling off and perhaps even declining a bit in some regions. However, there were differences in various ethnic groups.
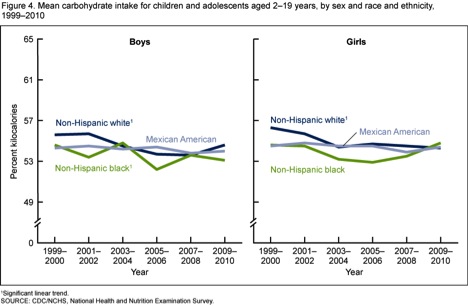
The next figure from the report shows that much of the change in overall calorie consumption is a result of a decline in carbohydrate consumption among whites. This might be a result of efforts to reduce the consumption of sugary drinks that are working in that subgroup or the population.
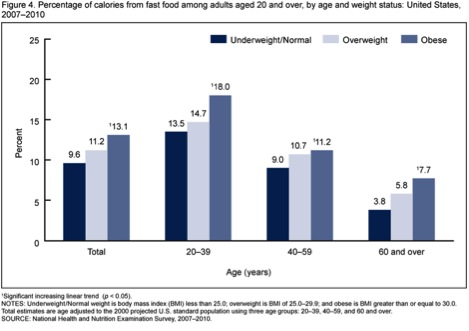
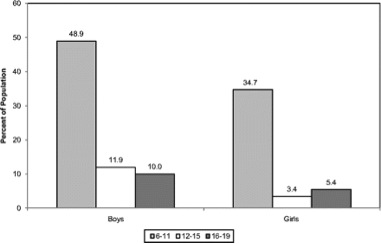
The second report is about adults and it focuses on who is eating how much fast food and what the impact of this consumption is on obesity. The next figure shows more fast food consumption by obese individuals in every age group. Again there are caveats with this data, but the message is pretty clear that consuming a lot of fast food is a big risk factor for obesity. If you want to read more about how people get addicted to certain types of food, here is a link to a long article from the New York Times on how the food industry has learned to develop products that really tickle our taste buds and leave us craving even more.
A Personal Experience & These Findings
I am somewhere between 6’4” and 6’5” (195 cm). At the end of August I weighed about 205 pounds (92.5kg). About that time my wife got the junk food (notably chips, crackers and ice cream) out of the house. I also started to limit my consumption of Dr. Pepper from about 1-2 cans per day to a couple per week and when hungry at work I now snack on either protein bars or apples and bananas. Since that time I have lost about 8 pounds (3.5kg). We were also pretty disciplined about having a few holiday treats, but after a cookie or two, trashing the rest. As you might imagine I am pretty physically active, but this time of year I am less active because I stop riding my bike to work when the roads get icy in November. So, this weight loss happened during a time of the year I have typically gained a couple of pounds (1kg) in the past, and I have seen a direct correlation between what the data in the charts tells us and my own body weight. The take home messages from all of this might go something like this:
- Groups and individuals who reduce their consumption of sugar and fast food/junk food lose weight, don’t gain weight, or don’t gain as much weight. All good things.
- If you are physically active, small changes in your diet can make a big, big difference. When in doubt have an apple. If you do get the junk food out of the house and moderate what you eat when not at home the weight seems to come right off.
- After a couple of months of change I don’t miss having a bowl of ice cream at night.
- Small changes over time make a big difference.
Good luck with your goals and I want to emphasize again that a collection of small changes over time can make a big difference whatever your goals.
Health Care Spending Facts & Sequestration
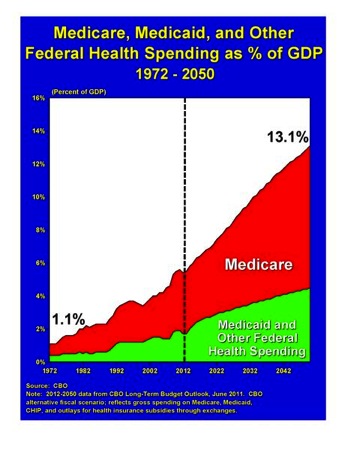
As part of the political trench warfare over taxes, spending and the long term federal debt the next big hurdle is so called “sequestration” on March 1st. If the President and Congress can’t agree on a combination of spending cuts and tax increases then a series of automatic cuts will take place. Behind all of this bickering is one simple fact. Medicare and other federal health care spending has risen from a tiny fraction of the federal budget to about 20% and is slated to continue to grow as the baby boomers retire. In this post I want to give you some background information via 5 slides that will be useful to frame later discussions about what to do about Medicare in specific and health care in general. The figure below comes from the Senate Budget Committee and shows key trends and future projections as a % of GDP. Also remember the U.S. spends a higher fraction of our GDP (about 18%) on health care than any country in the world.
Overall Health Care Spending
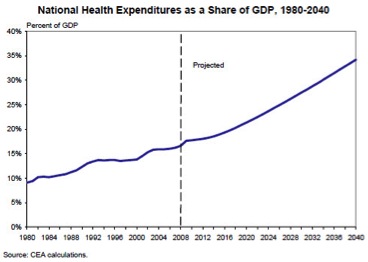
The next figure is from a White House report in 2008 (before Obamacare) and it shows what is projected to happen to total health care spending in the U.S. economy well into the future in the absence of significant “reform”.
An Unbiased Look at Medicare
For anyone want to take a deep dive into Medicare, the Kaiser Family Foundation has a series of slide shows on Medicare that cover almost every element of the program starting from the late 1960s. That having been said, I want to share three of the more than 120 slides posted on their website.
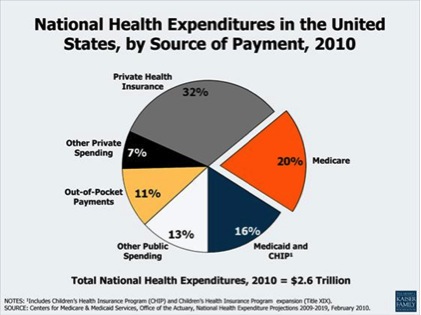
Kaiser Slide 1: “The Government” Pays 50% of the Bill.
The first slide is for anyone who has any doubt about just how much of the nation’s health care bill is paid for by the “government”. The magic number was roughly 50% in 2010 when you add up all programs (including employee benefits) at every level of government. So everyone needs to accept the fact the government involvement in health care is here to stay and we need to focus on how to deploy these resources in smarter ways.
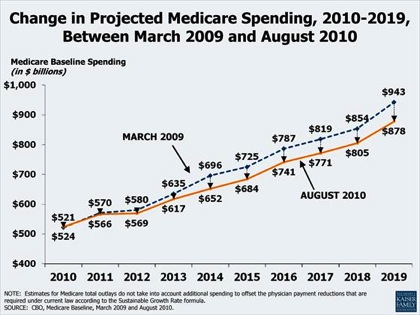
Kaiser Slide 2: Does Obamacare Bend the Cost Curve?
The next slide shows projected Medicare spending until 2019. The top line was pre Obamacare and the bottom line includes assumptions about costs savings as a result of it. The key point is that Obamacare does not move the needle that much. Additionally, the continuous upward trend shown in the 2008 White House slide above suggests that the many efforts at cost containment since 1980 have had limited effects on the growth of spending. In a later post I will discuss how much things like price controls, bundling, and potentially limiting access to technology have done so far when the “heavy hand of the Feds” has attempted to intervene to reduce the rise in health care spending (the short answer is not much).
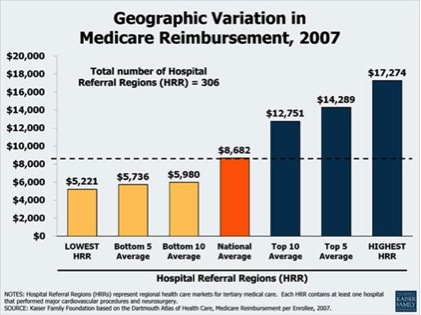
Kaiser Slide 3: Medicare Spending is All Over the Map!
The final slide shows how average Medicare spending varies more than threefold depending on where someone lives. The reasons for this variation have been debated and are complicated but overuse of services (e.g. doing things of little or no benefit to patients) is a major cause. This data also suggests that if more conservative and coordinated practice styles were adopted nationally there could be substantial cost savings for the country with no decrement in the quality of care provided to patients.
Summary
Health care spending in general and Medicare spending are complicated and emotional topics. The points I want to emphasize via the 5 slides above include:
- Spending is rising and the trends are not sustainable.
- The “government” is heavily involved in medical spending.
- There is wide regional variation in spending per patient that is not related to patient outcomes.
In future posts I will offer some ideas about what could be done to restrain government spending on medical care and help solve the long term budgetary challenges associated with these spending trends. Believe it or not there is one federal program that is a relative model of efficiency. More on that later, but there are models out there that work.
Bernard Lagat vs. Aging
Last weekend 38 year old Bernard Lagat, a multiple Olympic medalist in the 1500m, broke the American record for the indoor 2-mile run at the Millrose games in New York City. His time was just over 8:09. This prompted Nick Thompson of the New Yorker to post an excellent piece “Will Bernard Lagat Live Forever?” It highlighted a number of things about Lagat, a native of Kenya who now competes for the United States, and I was able to provide a bit of physiological insight for Mr. Thompson into why such a great performance was possible by such and “old” runner. In this post I want to take a bit of deeper dive into: a) just how unusual this performance is, b) some of the physiology behind it, and c) how long Lagat might continue to run fast.
A Fast Time by a 38 Year Old?
Every time someone in their late 30s or early 40s runs, swims, or rides a bike fast it causes a stir. That having been said the first thing to remember is that this is not unprecedented. Here is a top of my head list of other examples of people who have run very fast in their late 30s or early 40s (there are Wiki sites on all of these folks).
- Jack Foster – multiple fast marathons in his late 30s and early 40s.
- Carlos Lopes — 1984 Olympic marathon champ at age 37
- Francie Larrieu (Smith) – 5 time Olympian, last at age 40
- Steve Scott – broke 4 minutes for the mile 136 times, the last when he was 37
- Eamonn Coughlin – broke 4 minutes at age 41
- Haile Gebrselassie – set the world record for the marathon at age 35
- Miruts Yifter – gold medals in the 5k and 10k in 1980 when he as at least 36
- Constantina Diţă — won the Peking Marathon in 2008 at age 38
The 2-Mile Run is a Max Test!
It turns out a 2-mile run is essentially a VO2 max test and highly dependent on the maximum ability of the body to deliver oxygen to the exercising muscles. In fact the velocity at VO2 max on a flat incremental treadmill test to exhaustion is a great predictor of 3k or 2-mile time. This measurement also considers running economy because more efficient or economical runners will go faster while consuming a given amount of oxygen. The other thing to remember here is that while VO2 starts to fall at age 30 in untrained subjects it is both much higher and starts to fall later in the super fit who continue to train hard and do intervals.
What About Lagat, and How Fast for How Long?
Lagat is a relatively light trainer in terms of his weekly mileage, but he runs his mileage fast and does the type of interval training critical for maintaining a high VO2 max as you age. He also ran very fast indoor 3k times in 2010 and 2012, so fast times in races lasting about 8 minutes are nothing new. His relatively light training also probably protects him from physical injury and psychological burn out. All of this is consistent with information I shared in a previous post on running fast while getting older. So the only question is how much longer can these fast times last? The short answer is who knows, but longitudinal data on elite male distance runners over 20 plus years shows that those who continue to train intensely lose the least and those who train the hardest (not the most) lose almost nothing (2%) into their middle to late 40s. So, if Bernard Lagat wants to keep running fast, there is no physiological reason he can’t be running almost as fast as he is now for at least five more years. 1% of a fast 2-mile is about 5 seconds and somewhere under 8:20 would certainly seem possible for Lagat 5 years from now. He would only be 43!
Exercise, Cognition & Conscientiousness
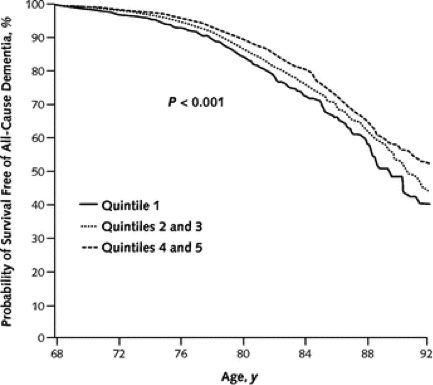
My last two posts have focused in part on the relationship between physical activity and cognitive function. Today I want to make two simple points and connect them. The first is from another Cooper Clinic database study and looks at the association between midlife physical fitness in about 20,000 people and a later diagnosis of dementia. The subjects were divided into fitness quintiles and followed for about 25 years. The figure below shows that individuals in the highest fitness quintiles had only about 64% of the risk of a dementia diagnosis compared to the least fit subject. Importantly, the level of exercise training needed to move up several fitness quintiles is modest and consistent with standard physical activity guidelines for adults, e.g. 150 minutes per week of vigorous walking.
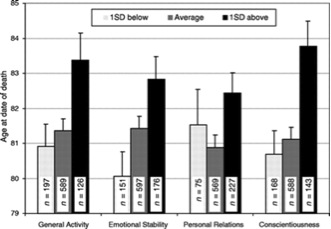
The second point I want to make is that a psychological trait known as conscientiousness is also associated with healthy aging and a modest increase in longevity. In a longitudinal study of aging conducted in about 2,400 residents of Baltimore, Maryland who were followed for five decades, people who scored high for conscientiousness lived longer. General activity, a marker of who is extroverted or “outgoing”, and emotional stability were also traits associated with living 2-3 years longer.
There are a couple of ways fitness and conscientiousness might be connected. The first is pretty straight forward and perhaps conscientious people just plain exercise more and generally follow health and lifestyle related guidelines about exercise, diet, not smoking and things like wearing seat belts. The second explanation is a bit more subtle and relates to the effects of exercise on something called executive functions. If exercise and physical activity enhance areas of the brain involved with executive functions — the ability to plan, stay on task, and pay attention — then people might be more likely to engage in healthy activities over time. If exercise helps maintain executive functions as we age then perhaps it is “easier” or more automatic for people to continue to stay fit as they age. So perhaps this is not so much about fixed personality traits as it is about exercise and conscientiousness reinforcing or amplifying a positive suite of behaviors over time.
None of this would surprise my grandmother who was born in the early 1900s and ultimately became a pioneer special education teacher in rural Indiana. She made sure all of her grandchildren and just about every other young person she came in contact with was exposed to books like The Little Engine That Could. I am sure she would not be surprised by the idea that good habits and a positive attitude generate more good habits and a positive attitude over time. To her that was a fundamental piece of Midwestern common sense.
Are Humans Going to Get Dumber?
This post is going to be discursive and ramble a bit, but bear with me and I think the ideas I am trying to integrate will come together for you. In my last post I reviewed some data about how exercise can improve academic achievement in kids along with the lifetime implications of physical fitness in childhood on brain health as we age. That got me thinking about a number of questions.
1. Will the world get dumber as people get less active?
Here is a figure from the American Heart Association showing the percent of kids in various age groups meeting the guidelines for daily physical activity. What will the long term implications of all of this inactivity be on the intelligence of society as a whole? Will all of this inactivity lead to a whole lot more fuzzy old people in the future suffering from various forms of cognitive impairment as they age?
2. What about forms of enrichment other than exercise?
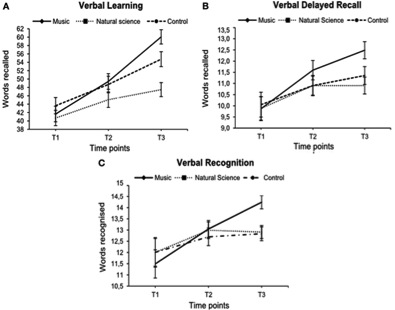
The data on the effects of school based music lessons on cognitive performance is pretty impressive, and music education early in life seems to have long lasting effects on the brain even if you don’t continue to play and practice into adulthood. The figure below is from the music lesson study that:
“….examined the effects of a school-based instrumental training program on the development of verbal and visual memory skills in primary school children. Participants either took part in a music program with weekly 45 min sessions of instrumental lessons in small groups at school, or they received extended natural science training. A third group of children did not receive additional training. Each child completed verbal and visual memory tests three times over a period of 18 months. Significant Group by Time interactions were found in the measures of verbal memory. Children in the music group showed greater improvements than children in the control groups after controlling for children’s socio-economic background, age, and IQ. No differences between groups were found in the visual memory tests. These findings are consistent with and extend previous research by suggesting that children receiving music training may benefit from improvements in their verbal memory skills.”
3. What about electronics?
The exercise and music lesson data might be interpreted in a very broad way to mean that doing things makes us smarter. Will the same apply for our interactions with the electronic environment that surrounds and invades us? This has been the topic of discussion in a number of venues and there are so-called smartphone holdouts who are worried that being connected to a computer will make them dumber. For example “in the old days” people used to routinely memorize phone numbers they called frequently. It seems to me that in the days of cell-phone speed dial and contact lists no one needs to memorize anything. Maybe this will just free up mind space for other things, or maybe it will make us dumber because our memory needs to be used and the ability to memorize trivial things is in fact a building block for higher order thinking and intellectual skills. In a similar vein, no one can do math in their head anymore……… those of us who grew up doing timed running or swimming workouts got very good at doing math in our heads as we calculated various split times and converted minutes to seconds depending the distance we were running or swimming. What about video games? A colleague of mine Dr. Bill Lanier commented that:
“My mother, who is a former college professor in education, says that if you only learn by having multi-modal input that incorporates sound, brilliant lights, movement, etc. (eg., video games), then you lose your ability to pick up a boring old book and envision what it is like to have characters move, speak, and interact.
Is the future a future with no memory, no math in our head, and no imagination?
4. Will electronics make us less active?
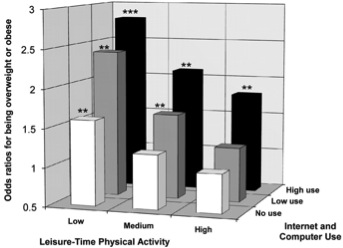
The figure below shows the interactions between screen time and physical activity and the odds of being overweight in adults. The authors of this study concluded:
“These findings suggest that, apart from nutritional and physical activity interventions, it may also be necessary to decrease time spent in sedentary behaviors, such as leisure-time Internet and computer use, in order to reduce the prevalence of overweight and obesity………Longitudinal studies are required to examine further the potential causal relationships between the development of overweight and specific sedentary behaviors such as Internet and computer use.”
I would add the combination of no physical activity and the frequently passive nature of the electronic environment could be a double hit to our collective intelligence for the reasons outlined above.
5. How much decision support is enough?
The ideas above are all about the negative interactions of physical and intellectual passivity. How far will this go? At some the level “the machines” are increasingly taking over both routine decisions via things like collision avoidance systems in cars, but the machines are also making us potentially passive bystanders in much more important things via so-called decision support. To take a bit of a leap, the recent debate on who decides about lethal military drone strikes highlights a number of issues about where this all might lead. Forget for the moment the moral and ethical issues associated with killing, what constitutes the battlefield, and who is a combatant. Imagine instead when the drones are programed with algorithms to support the remote pilots in deciding when to “pull the trigger”. The next step will be a statistical comparison of what the humans decided to do vs. what the algorithms “suggested”. What happens when there is no statistical difference? What happens if evidence emerges that is pitched in the context of the drones being “more reliable”. How soon until we give up life and death decisions to the algorithms?
6. The end of creativity?
Another issue with decision support is that it seems to me that it can be used primarily to make the known way or ways of doing things better. Imagine if decision support techniques had been applied to high jumping in the early 1960s. Detailed data on the biomechanics of how people jumped, their physical characteristics, and how they trained could all be collated and the ideal higher jumper could be identified and trained accordingly and incremental improvements made. But, what happened instead was as teenagers who “knew nothing”, Dick Fosbury and Debbie Brill, invented an entirely new way to jump that was revolutionary. The video below if of Dick Fosbury winning the gold medal in the high jump in 1968. Here is link to an extended to an interview with Fosbury.
click here for video
Summary:
I am not sure where all of this leads us, but I am sure that humans are designed to be mentally and physically active and we should be very careful both as individuals and a species about how much we stop doing at all levels. This includes being too physically inactive, having too much passive screen time, and turning over too many decisions to the machines.
LIKE MIKE

SUBSCRIBE TO RSS
