
Never Enough of Gary Player
A couple of months ago I highlighted Gary Player’s fitness regimen. At age 77 he is in the ESPN “body” issue. Here is a link to article on him and the video clip below show the great man in action.
click here for video

Health Care Costs:
It has been a while since I did a post on big picture issues related to health care in the U.S. In the last couple of months several ideas or perhaps rescue fantasies have emerged or perhaps re-emerged and I want to go over them.
1) Lack of Price Transparency
In the U.S. prices for various medical procedures are convoluted, idiosyncratic and extremely hard for even the experts to understand. A recent NY Times article on the costs of having a baby in the U.S. highlights many of these issues. Because there is no obvious rack rate and prices are not posted by most medical providers, some employers are essentially capping what they will pay for a given procedure or service. Along these lines, my bet is that there is going to be a big price transparency movement, more so-called bundled payments, and that the regulators will play a role in this. The important thing to remember is that what people and insurance plans actually pay typically has little relationship to what the list price is if you can find it. The other point here is that even if prices are more transparent it might not do that much to lower overall medical care costs which are driven in large part by utilization of services. I am all for more transparency, but it is not going to solve the cost problem. It is also interesting to note the late physician turned science fiction writer Michael Crichton raised many of these issues in a long article in the Atlantic published in 1970!
2) Rising Costs: a Problem Everywhere
The next point I want to make is that rising prices are a problem in almost all rich countries and a number of developing countries. Many of these countries have strict price controls and essentially government run programs. So thinking that there is some magical intervention “the government” can or should do to fix the problem is simplistic at best. My bet is that Obamacare will struggle to contain costs. The real drivers of rising costs are likely the aging population and advances in technology.
3) The Recent Slowing of Health Care Spending Growth
The rate of growth of health care spending has slowed recently. If this trend continues it has all sorts of implications for things like the U.S. Federal budget. However, I would urge caution in assuming that this trend will last forever. In past economic slowdowns there has also been a slowing of medical care spending growth followed by a rebound when the economy picked up. As I pointed out above no government in the developed world has effectively dealt with this issue over the long run, the population is still aging, and technology marches on.
4) Denial & Practice Variation
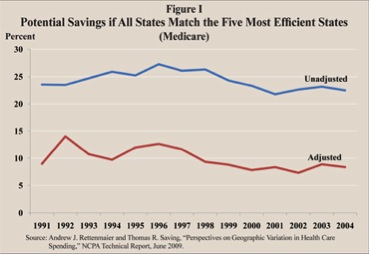
The current focus on price transparency and the recent slowing of spending growth are major distractions away from at least one major issue that might tend to reduce the rise in spending over time. That issue is the tremendous regional variation in the use of health care services in the U.S. and the lack of relationship between a number of markers of utilization and outcomes. Some argue that 30% of Medicare spending does not contribute to improved patient outcomes and is thus “wasted”. The figure below is a bit dated but still relevant and generally accurate. It shows a range of estimated savings for Medicare if all 50 States had utilization rates and practice patterns similar to the five most efficient States. Numbers in these general ranges likely apply to health care spending as a whole.
There are a number of ideas out there about how to deal with this issue, but they are likely to be challenging to implement.
5) Rent Seeking & Why This is Hard to Fix
Almost 18% percent of the GDP is spent on health care in the U.S. Almost 50% of this spending comes from the government in terms of either programs like Medicare or Medicaid, the VA, or Indian Health Service. Additional government spending is due to insurance provided to government workers at the Federal, State, and Local levels. There are also significant government subsidies for health care spending via the tax code. So, in one form or another “the government” probably covers 60-70% of medical costs in the U.S. As a result there is a huge and diverse group of vested interests angling for either maintaining or expanding their piece of this economic pie via what might be characterized as ‘rent seeking’ behavior:
“…..rent-seeking is an attempt to obtain economic rent by manipulating the social or political environment in which economic activities occur……”
Summary
Dealing with the high cost of health care in the U.S. is going to take more than price transparency and don’t bet the farm that current moderation of rising costs is going to last forever. The 800 pound Gorilla in the basement is utilization which, given the aging population, ever more technology, and economic incentives to over utilize, will be very difficult to contain.
Nelson Mandela & Resilience for 4th of July!
After the post on Alain Mimoun I got a nice note from publishing icon and fitness activist George Hirsch:
“Thanks for this. As a teenager, I attended the 1952 Helsinki Games and became a lifelong admirer of Mimoun, a true champion in every way.”
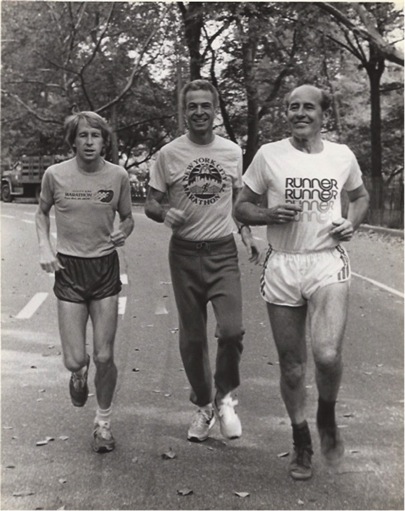
That led to a longer exchange about George’s role as a leader of the NY Marathon in bringing Mimoun’s great competitive partner Emil Zatopek to New York in 1979. The picture below is of Bill Rogers, George and Zatopek out for a run in Central Park.
As e-mail conversations sometimes do, things drifted to Zatopek’s support for greater political freedom as part of the Prague Spring in 1968. With the suppression of the Prague Spring, Zatopek lost his official status and was apparently given a series of menial jobs. At some level he was probably protected from even more harsh treatment by his international status and George Hirsch indicated that it did not take a major diplomatic effort to get him to New York in 1979. In 1990 he was politically “rehabilitated” as communism crumbled in the former Czechoslovakia. So, like Mimoun, Zatopek was a man of great personal resilience.
How Does This Relate to Nelson Mandela?
All of this discussion about resilience got me thinking about Nelson Mandela whose health and perhaps life is slipping away at age 94. The details of Mandela’s life are well known, but perhaps less well known is that he was devoted to a program of calisthenics and running in place during his nearly three decades as a political prisoner. In his 70s he then had the physical stamina to emerge from prison, lead his country and focus on reconciliation vs. revenge. He also continued an exercise program well into his 80s. I can’t help but think that his physical endurance contributed to his mental endurance and the resilience it took to just keep pushing forward against long odds. From a scientific perspective surely the exercise helped him deal with the stresses of resistance and leadership and kept him cognitively sharp for a long time.
The 4th of July is a time when we should all spend a few minutes reflecting about the ongoing struggle for human freedom. Thinking about how Nelson Mandela pressed on over so many years is a good place to start, and so is following his example and getting some exercise before the festivities and fireworks start. At some level resilience is a skill that can be learned and physical activity can surely contribute to it.
Alain Mimoun: Ahead of His Time
The great French/Algerian runner Alain Mimoun, who won the marathon at the 1956 Olympics, died last week at the age of 92. Mimoun is best known for his many silver medal finishes to the incomparable Emil Zatopek who is arguably the greatest distance runner of all time. Less well appreciated is that Mimoun is in many ways a herald of all that came after him:
- He was born in Algeria when it was still a French Colony. This is what we now might call the developing world and his excellence anticipated by more than a decade what other North African Arabs and runners from Ethiopia and Kenya have achieved starting with Abebe Bikila in 1960.
- He competed well for a very long time in an era when careers at the highest level typically lasted for only a few years. In 1960 he competed in his fourth Olympics and placed 34th in the marathon with a time of 2:31:20 at age 39.
- He won the French national title in 1966 at age 45 and in his early 50s he broke 2:35.
- He remained fit and active into his 90s.
I knew about his races with Zatopek and his victory in 1956 from the Bud Greenspan documentary “The Persistent Ones”, but I had no idea that he was one of the first great master athletes as well and a model for successful aging. The video below shows Mimoun running in the forest at about age 90. He was clearly a man ahead of his time and an example for us all.
click here for video
World Cup & Olympic Protests in Brazil
Brazil is slated to host the 2014 World Cup Soccer tournament and the 2016 Summer Olympics. Currently the FIFA Confederations Cup soccer tournament is being held there as a sort of dry run for these big events and the festivities have been marked by massive public protests over “spending on stadiums” vs. basic public service. The video below has gone viral and was posted a few weeks before the protests started.
click here for video
Mexico City 1968 and Denver 1976
The circumstances were different but there were large public protests including a massacre of about 40 protesters in early October of 1968 before the Mexico City Olympics. Here is a link to BBC reporting from that time and also a more recent review of what happened in Mexico City. In the early 1970s the people of Denver rejected public funding for the 1976 Winter Olympics, and the games were moved to Innsbruck, Austria. So, this is not the first time people have questioned the priorities associated with massive public spending on global sports extravaganzas.
Let Them Eat Stadiums?
Here is a link to an NYT op-ed piece entitled “Let Them Eat Soccer” with more on the situation in Brazil. I have been to Brazil a couple of times. It is a spectacular place poised to become a world power with world class people and capabilities in many areas. However, it is marked by all sorts of problems related to corruption, extremely high levels of social inequality, and just plain growing pains. In this context, is spending lavishly on stadiums a good idea? Similar questions have been raised in the US about public subsidies for professional sports stadiums which seem a bit crazy since the owners of the big sports franchises are typically “billionaires”. With people taking to the streets in Brazil and the ability of protests to go viral, I wonder what the long term effects will be on the ability of governments all over the world to subsidize stadiums. The recent US Open Golf Tournament at Merion also shows that extravagant purpose built venues are not essential to great competition. So, maybe there is a middle way.
Obesity: The “N” Word & Paula Deen
The celebrity “Southern” cook Paula Deen was essentially fired by the Food Network for bad behavior including use of the N word. In reading about this incident I ran across the picture below of loyal fans lined up outside her restaurant in Savannah, Georgia waiting to eat. The N word aside, this photo is a perfect example of the obesity epidemic in America, and raises the question of how and why we celebrate people who promulgate too much of a good tasting thing. Are there celebrity smoking and drinking advocates? Are there celebrity drive too fast advocates? Are there celebrity unsafe sex advocates? Do these folks, if they exist, get their own TV shows?

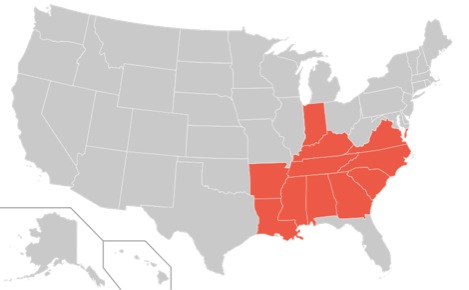
Southern Cooking & The “Stroke Belt”
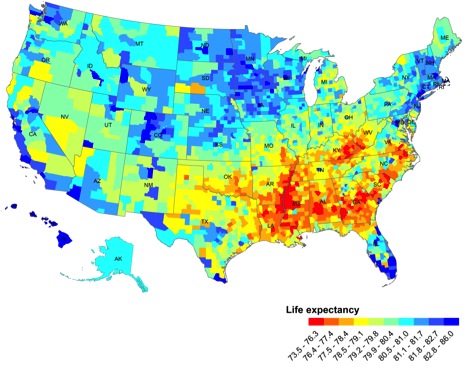
Diet matters and Southern Cooking and other unhealthy behaviors (smoking, inactivity, and obesity) have been implicated as causes of the so-called stroke belt which is shown in the first map below. It shows a region of the country where strokes are an especially big problem and other markers of public health are typically low. Obesity is also associated with about a 40% increase in health care costs that we all share one way of the other through health insurance premiums, taxes for programs like Medicare and Medicaid, or government disability payments. The second map shows the impact of these behaviors on life expectancy. The life expectancy data are confounded by things like poverty, race and education that seem to interact with all sorts of behavioral risk factors and determine who gets what disease and dies when. Paradoxically the data in the second map also shows that there are areas of the country with life expectancy values that rival those seen in places like Scandinavia and even Japan.
Summary
I am not sure we need to become a country of food puritans, but I do think we need recognize that these problems are not going to go away unless we do something, and cleaning up the countries diet, especially in the stroke belt might be a good start. The other interesting thing about the stroke belt is that it is a region of the country devoted to the rhetoric of “small government” and “individual responsibility”, but the data suggests that these philosophies are difficult for people to practice and that maybe Mayor Bloomberg is right. Denial is typically not a good policy and it is never a smart policy.
How Believable Are Running Records?
In my last post I discussed the recent analysis of how physiologically “believable” key mountain climbs by noted riders in the Tour de France have been over the last 30 or so years. The idea is doping likely contributed to some of the most unbelievable performances and that by analyzing power outputs, suspicious performances can be identified. That having been said, it is interesting to note that the one hour record for cycling has hardly budged since 1972 when Eddie Merckx went just over 49.4 km at Mexico City. People have gone much farther with exotic aero bikes, but the current record set in 2005 by Ondrej Sosenka is 49.7 km with a standard bike. Sosenka had a number of doping violations that ultimately ended his career, so this record is suspect. Merckx had issues with stimulants, but he rode in the pre-epo era and there is no evidence that I know of that he blood doped with traditional auto-transfusions. So perhaps his one hour record sets the gold standard for what is physiologically possible in cycling without manipulating oxygen transport using epo or blood doping.
All of this led to some interesting e-mail traffic and a discussion about what is physiologically believable in running. This is harder to guesstimate because unlike cycling, measuring the actual mechanical work done and power generated during running is very challenging. It is also harder to link running performances to estimates of oxygen consumption. However, one can ask what the best performance ever is in the pre blood-doping/EPO era was, use it as a baseline and then go from there. This is reasonable at some level because by the 1960s people were training as hard as they do now, and lab data from that time suggests the record holders then were comparable to today’s top performers. Additionally, the first real suspicions of blood doping emerged with Lasse Viren in 1972 and 1976. Here is an example using men’s marathon and 10,000m performances:
- Derek Clayton ran 2:08:33 in 1969 and his best for 10k was relatively slow 28:45 (likely on dirt). In that era the fast 5,000 and 10,000m runners did not move up to the marathon that often, and if they did it was at the end of their careers. There was no real money to be made running and the races (except for Boston and the Olympics) were pretty low profile. Clayton’s record lasted 12 years until shortly after the big city/big money marathons started and top track runners “moved up”. So people with 10k PRs faster than Clayton started to run the marathon and they started to run more of them at the peak of their careers.
- The fastest 10k time on dirt is 27:39 by Ron Clarke in 1965. If you figure a synthetic track is worth 2-3% then Clarke might have run ~27:00 on a synthetic track. This time is equal to about a 2:04 for the marathon if you plug it into one of the better race conversion calculators. Clarke ran his 27:39 alone and like Jim Ryun’s 3:51:1 mile on dirt there was not a pacer. Both would have run faster in a real race with a pacer.
- There are about 50 people who have broken 27:00 for 10,000m, the fastest time since drug testing got “better” over the last 5 or so years is about 26:45. Many of the rest of the best times are from the mid-90s to about 2005 when epo was endemic. Bjarne Riis used epo in the 1993 Tour de France and it is hard to imagine that the runners were far behind. There is also evidence that the East Africans are not as clean as widely believed, and throughout this period they had managers and trainers from the same parts of Europe noted for doping in cycling.
- So it looks like a human might be able to run 26:45 with limited suspicion of doping and that works out to about a 2:03:03 estimated marathon. If 26:30 is possible without drugs you get 2:01:54. 26:20 gets you 2:01:08. The race conversion calculators are not perfect but they are pretty good and most of them (plus an old point table system from the early 70s that I have a hard copy of) give relatively convergent estimates.
- You can do a similar analysis (with a dirt track conversion factor) for the mile, 3000m and 5000m and the records from the middle 60s look very similar to those up to about 1990. Also the best performances since about 2008-10 (when drug testing got better) are slower than the current records and perhaps closer to the pre-doping values.
Ultimately, who knows which runner has been doing what over the last 20 or so years? Who ran what race clean, who doped, and who was clean all of the time and who doped all of the time. However, like the hour ride for Merckx, there is no evidence that the current elite runners are physiologically better than people from an earlier era when techniques to manipulate oxygen transport for a competitive edge were not available.
Is Obesity a Disease?
The recent and controversial AMA decision to categorize obesity as a disease has a raised a number of questions and discussion points. I thought I would cover a few here to help readers sort through the issue on their own.
Definition of Disease
Below is an extended quote from the wiki definition of disease. It is similar to other definitions I found and if you link to the site there is a pretty comprehensive discussion of the concept of disease and related things like “disorder” or syndrome. Based on the blurb below obesity certainly seems to fit many of the definitions of a disease. One interesting recent observation is that if you track obesity in social groups it moves through them with a pattern that looks a lot like the way infectious disease moves through a population.
“A disease is an abnormal condition that affects the body of an organism. It is often construed as a medical condition associated with specific symptoms and signs.[1] It may be caused by factors originally from an external source, such as infectious disease, or it may be caused by internal dysfunctions, such as autoimmune diseases. In humans, “disease” is often used more broadly to refer to any condition that causes pain, dysfunction, distress, social problems, or death to the person afflicted, or similar problems for those in contact with the person. In this broader sense, it sometimes includes injuries, disabilities, disorders, syndromes, infections, isolated symptoms, deviant behaviors, and atypical variations of structure and function, while in other contexts and for other purposes these may be considered distinguishable categories. Diseases usually affect people not only physically, but also emotionally, as contracting and living with many diseases can alter one’s perspective on life, and their personality.”
Defining Obesity
BMI or body mass index has emerged as a favored definition of obesity. This definition is probably OK when thinking about groups or populations of people but does not always tell you much about an individual. There can be “normal weight” people with a lot body fat and health problems, and there can be heavy people with lots of muscle mass and very little body fat. Then there is the problem of distribution of fat. Visceral fat or “belly fat” is worse for your health than fat in your lower extremities. When I started medical school in the early 80s fat was seen mostly as a tissue that simply stored excess energy, but in the last 20 or so years it turns out that some fat cells secrete all sorts of biologically active substances that wreak havoc on the blood vessels, heart, liver, pancreas, skeletal muscle and brain. One critical thing to note is the physically active “fat people” are largely protected from some or most of these problems
What Does Disease “Status” Do?
The AMA decision does not do anything right away other than make a statement and raise a bunch of questions:
- Will disease status increase public awareness of obesity as a medical problem? My guess is that most people are probably already aware that obesity is a problem.
- Will disease change medical practice and encourage more Drs. to discuss the issue with patients? Should things like exercise and physical activity be a vital sign?
- Will disease status influence the way insurance covers certain treatments like gastric bypass? Some plans do, some don’t and here is link to a nice opinion piece on that topic. What happens if the insurance plans that political leaders get cover it but not the plans the rest of us have?
- Will disease status limit the use of sin taxes and incentive plans linked to weight loss by governments and insurance companies?
- Will disease status encourage people to take more or less responsibility for their own behavior? Obesity is a lot more than a few bad genes “making us fat”. In fact genetics likely plays a minor role for most people and the big increase in average body in the US over the last couple of generations has occurred faster than any genetic changes that might explain it. For the vast majority of us it is all about the environment and our behavior.
Our Obesogenic World!
We live in a high calorie low physical activity world primed to make us all fat. At some level it is amazing that anyone remains normal weight. The lessons from improved traffic safety and smoking rates over the last 50 plus years tell us that these big public health problems require structural changes in society as well as changes in individual behavior and so-called “choice”. Where to start with the obesity problem: Sugar and fat taxes or other policies designed to reduce calorie consumption and increase healthy food choices? Walking and biking friendly urban planning? Safe streets to encourage getting outside in all neighborhoods? More PE and better nutrition at school? Financial incentives via health insurance plans? Limiting our own screen time and that of our kids? Drs. and nurses communicating more about the problem with patients with easier referrals to diet and exercise programs? The short answer is all of the above.
LIKE MIKE

SUBSCRIBE TO RSS
