
Talent, Talent, Who’s Got The Talent?
Have you ever gotten into a long three or four way e-mail conversation with friends and colleagues? Recently I had one that started out on the topic of “talent identification” in sports and headed off into several related directions over multiple days. In addition to me, the participants were David Epstein, the author of the “Sports Gene”, Terry Laughlin, the creator of Total Immersion Swimming, and the runner/author Amby Burfoot. Here is a synopsis of some of the things that came up in the exchange.
1.) The Kid From Fargo
The conversation started when I asked David, Terry and Amby what they thought about the following story. On the day after Christmas, my wife and I did a short swim workout at our local athletic club. The next lane was occupied by a young guy who was doing what might be described as a serious swim workout. During a break in his interval training, I asked what college he swam for thinking that perhaps he was a small college swimmer home for winter break. Instead I learned he was high school kid from Fargo, N.D. visiting relatives in Minnesota. We talked a bit more and he told me he could break 1:50 for a 200yd freestyle. He also did some running with a 2-mile best of around 9:50. His training regimen sounded serious but modest with no year round running for example. I also guessed that the mystery swimmer was about 5’10” (9180cm) and 150lbs. (68 kg)…….perfect size for the triathlon. We finished the conversation with me encouraging him to give the triathlon a try.
So, how good could the kid from Fargo get if he trained seriously for say an Olympic distance (1500m swim, 40km bike ride, and 10km run) triathlon? The fact that he was training alone while on vacation made me think he was pretty committed. His times while very good are not great; however, Fargo is not an endurance sports hotbed and who knows what opportunities he might have to really train and improve in college. My bet is that with training he could become at least a sub-elite regional class triathlete, and with a bit of luck perhaps national or even world class.
2.) Talent Identification
I have made the point before that in comparison to a country like Kenya there is plenty of wasted aerobic talent in the U.S. The other critical point is that talent identification works. A good recent example is the Great Britain Rowing Team Start Programme which seeks to find tall people with a lot of aerobic power and turn them into rowers. This effort has been successful and resulted in a number of Olympic medals and World Champions and there is also a focus on who is motivated to do the training required to excel:
“The right physical characteristics are of course not the only factor that is needed to achieve that ultimate prize of an Olympic gold medal. You also need commitment, the ability to train hard and the right mental attitude. Even with all the physical capabilities described above if you don’t make the full commitment to training and make sacrifices where necessary then even the most talented person will not make it.”
So, when you say lack of talent, my response is lack of talent identification.
3.) What About Motivation
In our e-mail exchange Terry pointed to an experience about motivation that he had early in his coaching career that I found fascinating:
“The most interesting observation I made while working with younger competitive swimmers–including a fair few elites who I developed–was that intrinsic motivation was a far more significant factor than physical talent. I first noticed this accidentally because my first coaching position was at the U.S. Merchant Marine Academy at Kings Point, 1972-75.
But the much more interesting observation was about motivation.
At Kings Point everyone was on scholarship, so no one swam for that reason. That left two reasons to swim (1) You wanted to, and (2) You did so to escape shit duty, as athletes were excused from reviews, washing latrines, swabbing floors, etc, during the season.. The prevalence of people who swam for intrinsic reasons in the faster lanes, and of escapers in the slower lanes, was even more striking than of body types. That observation remained true for the rest of my career in ‘serious’ coaching which continued through 1988. And it remains the most influential aspect of the coaching I’ve done since.”
4.) Early Specialization: Good or Bad?
One of the big ideas out there is that champions in sport and elites in many fields are made and not born via 10,000 hours of deliberate practice. This would tend to argue for early specialization. However, David pointed out that for “CGS” sports that are contested in centimeters, grams, or seconds there is evidence that later specialization is better:
“Based on a Danish sample of 148 elite and 95 near-elite athletes from cgs sports (sports measured in centimeters, grams, or seconds), the present study investigates group differences concerning accumulated practice hours during the early stages of the career, involvement in other sports, career development, as well as determining whether or not these variables predict membership in the elite group. The results clearly reveal that elite athletes specialized at a later age and trained less in childhood. However, elite athletes were shown to intensify their training regime during late adolescence more than their near-elite peers. The involvement in other sports neither differs between the groups nor predicts success. It can be concluded that factors related to the organization of practice during the mid-teens seem to be crucial for international success within cgs sports. Future research should adopt a longitudinal design with means of drawing causal inferences.”
Did the late specializers do better because they intensified their training during a key period of physiological growth and development? Did being a bit older allow the most motivated kids to pick the sport that interested them the most and then really commit to the required training for the internal vs. external reasons mentioned by Terry above?
There is a lot of talk about of how birthdays early in the year are key determinants of who does well in sports like Hockey via what is called the relative age effect. The idea is that kids who are relatively older do well and thus get more ice time and practice and thus get better and better leaving the younger kids in the dust. However, on further review this appears to be a superficial analysis:
“Because RAEs are well-established in hockey, we analyzed National Hockey League (NHL) drafts from 1980 to 2006. Compared to those born in the first quarter (i.e., January-March), those born in the third and fourth quarters were drafted more than 40 slots later than their productivity warranted, and they were roughly twice as likely to reach career benchmarks, such as 400 games played or 200 points scored. This selection bias in drafting did not decrease over time, apparently continues to occur, and reduces the playing opportunities of relatively younger players. This bias is remarkable because it is exhibited by professional decision makers evaluating adults in a context where RAEs have been widely publicized. Thus, selection bias based on relative age may be pervasive.”
There are other holes in the 10,000 hour argument that David has covered in his book. It is certainly an interesting idea that is easy to grasp, but like a lot of ideas that are easy to grasp sometimes the nuances get lost as things get oversimplified for public consumption.
5.) Limits of Deliberate Practice?
Amby wanted to know what happens to people that really devote themselves to something new later in life. The example of Dan McLaughlin comes to mind. Mr. McLaughlin essentially quit his day job as a commercial photographer to see just how good a golfer he could become with 10,000s of deliberate practice:
“On April 5th, 2010, Dan quit his day job as a commercial photographer and began The Dan Plan. Having never played 18 holes of golf in his life, Dan started the 10,000 hour journey with just a putter. After five months of putting, he received his second club, a pitching wedge. Just before the first anniversary of The Dan Plan, Dan took his first full-swing lesson. After 18 months he swung a driver for the first time. On December 28, 2011 he played his first full round with a full set of clubs. Since then it has been off to the races.
Logging in 30-plus hours a week he will hit the 10,000 hour milestone by December 2016. During this time, Dan plans to develop his skills through deliberate practice, eventually winning amateur events and obtaining his PGA Tour card through a successful appearance in the PGA Tour’s Qualifying School.”
From what I can tell, three years into his plan, Dan McLaughlin currently has a handicap of about 6 meaning he usually shoots about six over par. I am not an expert on handicap systems but from what I can tell top PGA pros are routinely a few shots under par on their home courses. At some level this little experiment shows us both the power and limits of deliberate practice. Dan McGlaughlin is becoming a solid golfer and now is in the 10% of people who actually take the time to post handicaps. To put it in perspective, about 15% of marathon finishers run under 3:30.
However, I would be remiss if I did not highlight that many positive aspects of deliberate practice including improved performance and learning how to spend more time in a relaxed Flow like state while doing challenging things. These effects can be hard to quantify but as Terry points out most of the time the key is train well vs. simply harder.
6.) The Talent Question
To become truly skilled at most things requires practice. Practice plus the nebulous concept of talent can lead to exceptional performances. David tells me that the Kenyan runners are convinced they are more talented. Is this real? Does their belief increase their motivation and lead the most talented kids to pursue running? Does it give them a psychological edge in competition? Or, do they end up simply training harder as a result of their beliefs?
Based on everything I know, most tests of talent are pretty crude especially when you are trying to find the most exceptional person in a field full of exceptional performers. This is true for tests in the physiology lab, paper and pencil tests of academic performance and also genetic testing for most things. The tests needed to determine who has 1/100 talent, 1/1,000 talent, and 1/10,000 just are not there. That having been said, the great NFL quaterback Tom Brady was a 6th round draft pick with marginal NFL combine scores. Does the fact he got to the NFL combine mean he was exceptional? Or, does the mismatch between his “test scores” and performance simply show just how hard it is to determine or predict objectively who will be the best of the best?
Finally, to the extent that talent is something innate we don’t have control over it. However, we do have control over how we apply it and I hope the kid from Fargo sees what he can do.

Did The Future Begin in 1980?
I thought it might be fun to do an end of 2013 post on the “future”. However, as I looked for interesting graphics about the current world and where we might be headed, it occurred to me that the future as we know it (and as it is likely to emerge) really started in about 1980. Here are some examples:
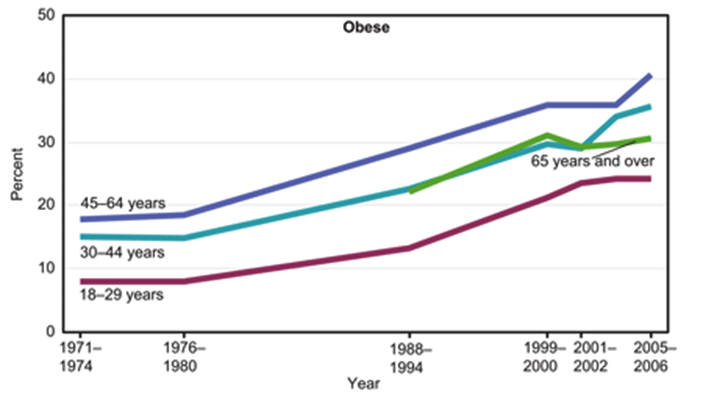
1. Obesity
The US in specific (and the world in general) is fatter than ever. This trend started in the US in about 1980 and other countries are now “catching up”.
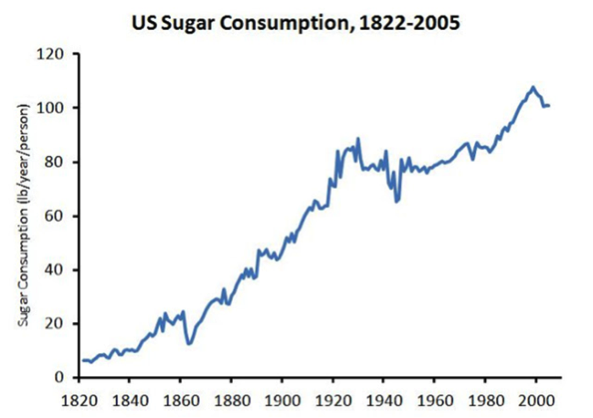
About the same time sugar consumption started to increase as well above levels that had been stable from about 1920-1980. This has largely been due to high fructose corn sweetners. Some argue that this increased sugar consumption is “the cause” of the obesity epidemic. The view I favor is that it is emblematic of rise in processed food and calorie consumption, more screen time, and less physical activity.
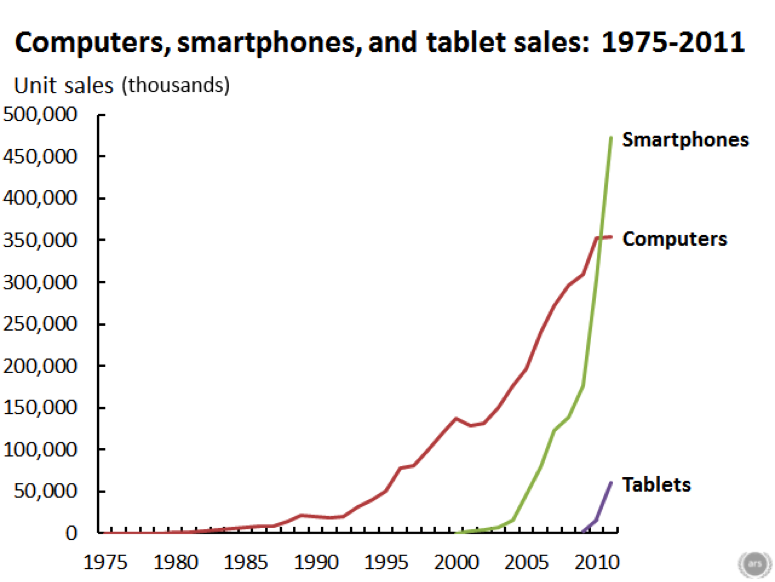
Speaking of screen time, below is a graph that shows the rise in consumer electronics over the last 30 plus years. Like obesity rates and sugar consumption, things started to change about 1980.
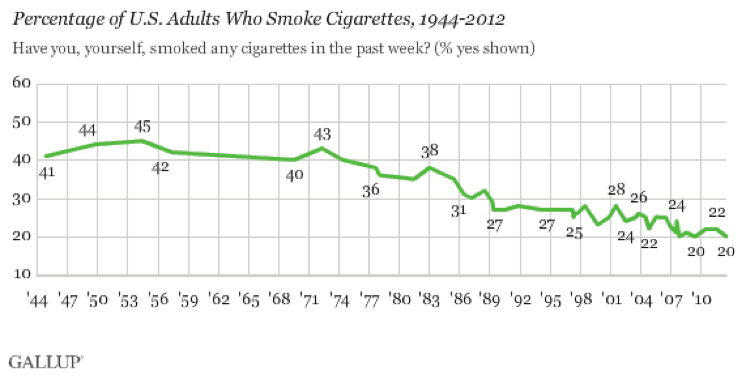
2. Smoking
While obesity, too much processed food, and ever more screen time there are making us less healthy there is at least some good news – smoking rates are at an all-time low. There was some downward movement in the 70s, but things really started to drop in about 1980.
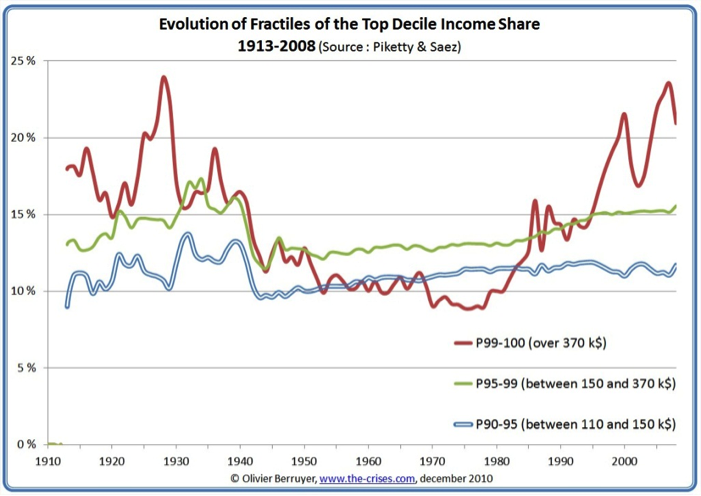
3. It’s the Economy Stupid
The big things you hear about related to the economy focus on things like income inequality, globalization and the loss of manufacturing jobs in the US. Again, none of this is new and if you look at the chart below you see that the fraction of total income (red line) going to people in the top 1% has doubled since about 1980.
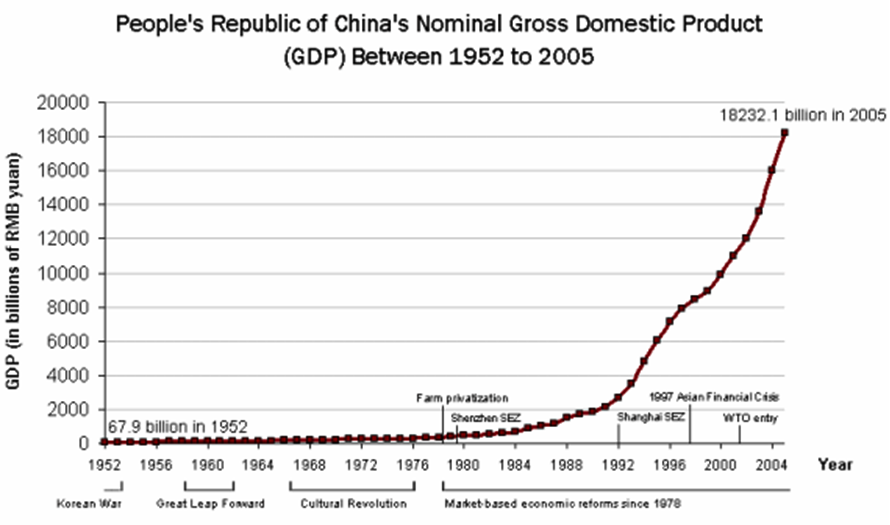
The next chart shows what has happened to China’s economy since 1980.
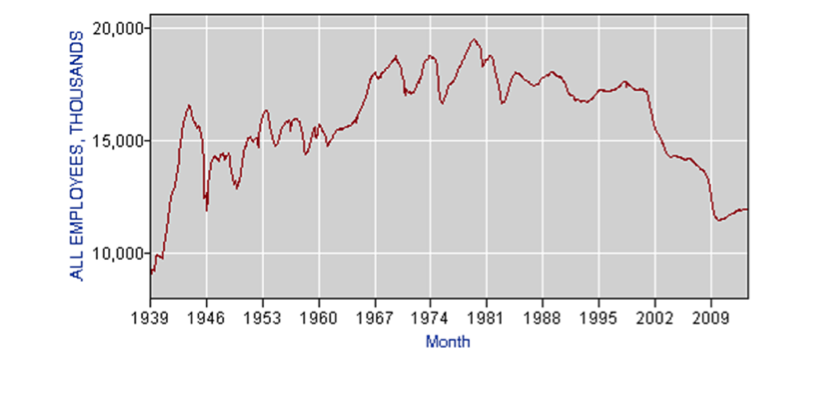
US manufacturing jobs trended upwards in the post WW2 era until about 1980 and have since declined pretty dramatically. The next chart shows the total number of manufacturing jobs in thousands.
For those who seek a single cause for the rise income inequality it would is easy to make a simple conclusion that income inequality was “caused” by either globalization or the loss of manufacturing jobs since 1980. However, like obesity, the cause has probably been multifactorial but it is hard to believe that globalization and loss of manufacturing jobs were not major contributors. It is also interesting to think about the effects of the electronic environment on jobs as machines and computers do more and more things.
4. The Future of The Future?
So perhaps the future is a fatter, screen time driven world with more economic disparity. Or maybe there is nothing new and that version of the future has been with us since about 1980? The one new trend that will have a both a national and world wide impact (at least as big as the seven charts above) is the aging of population. The final chart shows the ratio of people over 65 to the number of people between 15 and 65 in the US. Things start to take off in about 2010 as the baby boom generation starts to hit retirement age.
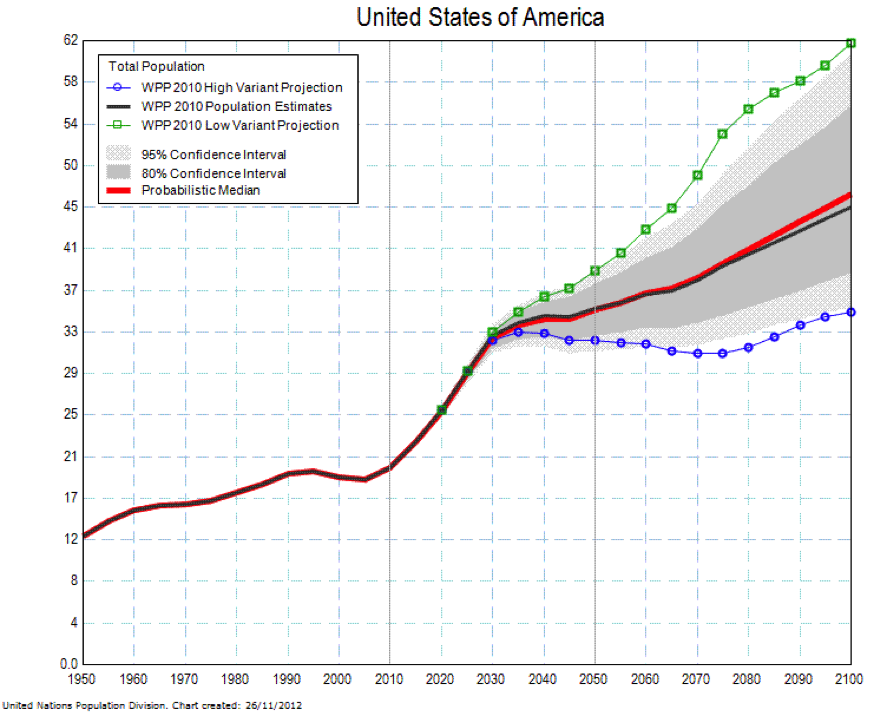
Look at the chart and ask yourself what will the world look like when there are more older than younger people? Will the pension and medical care costs caused by aging bankrupt whole countries? Is a rise in the retirement age unavoidable as a result of this new demographic reality? What constitutes “fair” for government spending and tax policies? The first seven charts are a look back and what they report was probably unanticipated by most people in 1980. The final chart shows a trend that will almost certainly happen and that we need to prepare for.
Statins, 23andMe, and Personalized Medicine
What opinion leaders in biomedical research were thinking 20 or 30 years ago seems pretty remote from the news last month that the American College of Cardiology and American Heart Association released new guidelines on statin therapy to reduce the risk of cardiovascular disease. It also seems pretty remote from the more recent news that the FDA told the genetic screening company 23andME to suspend their direct to consumer health related genetics testing and advice. At first glance these two stories are unrelated, but bear with me while I make the case that both stories are fundamentally about the limitations of something called personalized medicine and the routine use of genetic testing to customize therapy for individual patients.
Statin Guidelines
The net effect of the guidelines is to recommend that far more apparently healthy people be treated with statins to prevent cardiovascular disease. The new guidelines have been controversial from the start and criticized for reasons including: 1) what data and studies were used to develop the guidelines, 2) the accuracy of the calculator used to estimate who is at what risk and in need of treatment, and 3) the deemphasizing of cholesterol monitoring to adjust therapy. There was also yapping about links between some of the guideline writers with the pharmaceutical industry and just the confusion associated with changing recommendations on how commonly used drugs should be used. What most people fail to realize when they read about the next best medical thing is that medical evidence and recommendations shift and change over time. In a recent review of how medical evidence changes more than a third of what is considered state of the art underwent significant challenge or revision over 10 years. So the fact that the new statin guidelines are controversial and why they are controversial is not surprising.
Direct to Consumer Genetics Testing
23andMe was essentially banned from offering to direct consumer information about disease risk based on genetic testing. The main concerns outlined by the FDA relate to the basic validity and reliability of the testing, how assessments of risk were being communicated to the consumer, and the unpredictable nature of how a consumer might respond to a “positive” test. For common non-communicable diseases (the stuff the kills most of us like diabetes, cardiovascular disease, obesity, and many forms of cancer) there are hundreds of gene variants that put people at increased risk. However the increased risk for each variant is typically tiny and pales in comparison to behavioral risks much of the population engages in. In reality no one really has a good handle on the real risk associated with most gene variants and there is much less insight into how they should influence medical decision making. The other dirty little secret here is that it has been difficult to replicate risk variants across studies, and for a number of diseases the gene variant profiles are the same in people with and without the clinical disease. There are also the predictable issues of what findings in one ethnic group might mean in a different group.
Not so Fast: The Statin 23andME Link
Sometime in the 1980s or early 90s the idea took hold that if we simply knew enough about the individual genetic profile of each person that we would be able to customize drug therapy in specific and medical therapy in general to better treat, predict, and prevent a wide variety of disease. Most prominent academic medical centers now have huge programs based on this basic proposition. The FDA’s message to 23andME can be viewed as a “not so fast” message. Whoever is doing the testing, there is a lot left to learn before personalized medicine might really make a difference for most people seeking advice from most Drs. for most of what ails us.
In this context, the statin guidelines say the same thing the FDA did by what they don’t recommend. Instead of recommending that statin therapy be tailored based on each patients genetic profile and cholesterol level, they advocate use of a generic risk calculator derived from decades old epidemiology studies and then largely abandon the idea that it is important to follow how the drugs affect cholesterol levels. Maybe the next step is simply putting statins in the water.
As far as personalized medicine in general goes, research might ultimately get us to a genetically based diagnostic and therapeutic promised land. However, don’t be surprised if personalized medicine based on your individual genetic profiles ends up becoming the biomedical version of atomic fusion, an attractive idea that just can’t quite get there for most diseases.
Sleep & Health
The usual article on sleep and health focuses on how we are all sleep deprived and the bad things this does to us. The story is pretty simple: chronic low grade sleep deprivation leads to systemic inflammation, weight gain, excessive eating, and hormonal changes that are associated with all sorts of long term health issues. The drowsiness also leads to poor judgment, more accidents, more eating and other shorter term issues. This is all being made worse as technology ranging from artificial lighting to smartphones that make our days longer and longer. Many of us then get up earlier and jump start the day with a mega dose of caffeine.
The epidemiologists tell us that 7-8 hours per day of sleep is the optimal health sweet spot for most of us. People who routinely get by on 5-6 hours of sleep have about 1.5 times the relative risk of death from coronary heart disease. Interestingly, the risk is about 1.4 times for those who sleep a lot:
“Too little or too much sleep are associated with adverse health outcomes, including total mortality, type 2 diabetes, hypertension, respiratory disorders, obesity in both children and adults, and poor self-rated health. The relationship between duration of sleep and vascular events is U-shaped, suggesting that different mechanisms may operate at either end of the distribution of sleep duration.”
If you are worried that you are getting either too little or too much sleep there are some simple steps you can take that work for most people to promote better quality sleep. Highlights include:
- Avoid napping
- Limit the use of (caffeine) to earlier in the day
- Morning exercise
- Avoid large meals before bedtime
- Get adequate exposure to natural light
- Establish a bedtime routine
- Use your bed for sleeping as opposed to reading and watching TV
- Make where you sleep a comfortable place
As a result primarily of the obesity epidemic there is also an epidemic of sleep disturbed breathing. There is a simple questionnaire that can help determine if you have the problem and need medical follow-up.
Sleep & Exercise Performance
What about short term sleep deprivation and exercise performance? What happens when you have a competition and only get four hours of sleep the night before? What if you are in a multi-day event with little time for sleep? Many of the studies on this topic are from the 1980s and 90s and they tend to show that even 30 hours of total sleep deprivation does not do much to VO2max. Studies on longer term submaximal exercise are limited but they tend to show exercise time to exhaustion is reduced but with some subjects effected far more than others. One general finding appears to be that people rate whatever they are doing as harder to do when sleep deprived.
Countermeasures
An interesting source of data on exercise performance and sleep deprivation comes for the literature on physical conditioning and military Special Forces. These individuals frequently do very demanding night operations for several nights in a row with limited opportunities for daytime sleep. In a series of Canadian studies that simulated several days of night operations, caffeine (1-200 mg) improved run time, cognitive performance, and marksmanship.
Another interesting idea is that recovery from days in a row of vigorous activity with short sleep can be enhanced by protein supplementation. There is a lot of discussion in military nutrition circles about 20-25 gms of protein before sleep during periods of high stress physical activity. The idea is that muscle mass will be better preserved during periods of physical stress, sleep deprivation, and limited calorie intake. It would be interesting to know if professional cyclists are adopting similar strategies during the big stage races.
Closing Thought
As part of my medical training I have probably spent more time than most people both working and working out while sleep deprived. There are short term strategies to deal with it, but sleep deprivation is no fun and my goal in middle age is to avoid it as much as possible. Advice that is easier to give but harder to act on in our high strung world.
A Deep Dive & Risk
Last weekend there was a “60 Minutes” segment on the emerging sport of free diving. That plus the death of free diver Nicholas Mevoli got me thinking about risk and extreme sports. When things like this happen sometimes I get calls from the press and almost always my physician colleagues want to know “why anyone would try these things?” Here are the ideas I cover in response to that question.
The Power of a Subculture
People who attempt to set extreme records or push themselves to the limit are usually part of an extreme and somewhat closed subculture. Their friends and peer group share an intense interest in an activity and it becomes literally what they eat, breath and dream about. A question like “how are you today?” from a casual friend or co-worker is frequently answered with something like “pretty good, I did a hard 15 mile run first thing this morning, we will see how the 10 miler this afternoon goes.” This might be seen as an odd response in the real world, but totally normal in an extreme athletic subculture.
That sort of dialogue is an example from running but similar discussions can be had with those who are really committed to just about anything. If you have never been part of an extreme athletic subculture three books that describe them in detail are “Muscle”, “Once a Runner”, and the recent the “Secret Race” by Tour de France rider Tyler Hamilton. So, there is plenty of social reinforcement to “go for it” from the subcultures that people who are committed live in.
My Neurotransmitters Made Me Do It
One of the hallmarks of traditional addiction is the need to use ever more external stimulus to get the same satisfaction from whatever you are addicted too. Traditional addiction to drugs rewires brain circuitry and neurochemistry to make this happen and there is evidence that gambling can do the same thing to susceptible individuals. For many a peak and intense athletic experience is sometimes followed by a letdown as the excitement associated with the planning, training, and anticipation of the big event vanish afterward. The obvious solution to this problem is to find an incremental challenge and start the whole process again. Parallels with gambling seem appropriate here and when you mix what is happening in the brain with the right subculture it is pretty easy to see how the need to do ever more extreme things happens.
The Environment
A lot of disasters and deaths occur in extreme environments. Think altitude, diving, hot and cold. There are tremendous physiological adaptations that can be activated both acutely and in response to training that help us do more or go longer in extreme environments, but when things fail they can fail catastrophically. There is a quote about bankruptcy from the “Sun Also Rises” by Earnest Hemingway that applies to physiological responses to extreme challenges:
“How did you go bankrupt? Two ways. Gradually, then suddenly.”
A classic example of this is watching soldiers faint while at attention on a hot day or seeing a patient respond to potentially life threatening blood loss. If you were to measure the vital signs they would be pretty normal until just before loss of consciousness when there is a sudden drop in blood pressure. When this happens many of the physiological systems that are compensating for the challenges of not enough blood returning to the heart fail essentially at the same time. You can tell a similar story about catastrophic physiological failure in response to other severe stresses as well. So, people feel OK until they don’t and in extreme environments the distance between OK and death is not that far.
You Are On Your Own
Of the people injured in the Boston Marathon bombing essentially everyone who made it to the hospital alive survived. This is one of the main lessons from military combat casualty care for civilian medicine. Extreme sports take place in extreme environments distant from the types of comprehensive medical care that make an incredible array of injuries and illnesses survivable especially in young otherwise healthy patients. Other things that come to mind are the availability (or lack thereof) of specific equipment and logistical support needed to do challenging things in a safer way. Getting a lot of hardware and a support crew to a remote location is challenging and sometimes there might be a temptation to try to do more with less.
Risk Amplifies
Extreme environments, the limits of physiology, and logistical issues are all risks but they are all amplified by poor judgment. I like to tell people that taking four 3% risks at the same time doesn’t mean you have a 12% risk of failure. Instead the risk is more like 3x3x3x3 or 81%. This is a theoretical example but things really do seem to multiply while doing extreme things in extreme environments. Time and time again you hear about people choosing to push it just a bit more prior to a disaster.
I Am All For It
Based on the observations above you might think I oppose people taking on extreme challenges in fact I am all for it. Back in 2011 when Diana Niad was attempting to swim from Cuba to Florida I commented to PBS that questions about “why” do it
“miss the point, at some level, you’ve got to admire anybody who wants to test the limits of human potential in general, and her own limits, in specific…It’s a good thing we’re not all average.”
That having been said, I just want people to understand what they are getting into and avoid getting sucked up by their subculture and neurochemistry into challenges they are not prepared for in truly unforgiving environments.
Who’s Doping Now?
For most of us when I say doping you say Lance Armstrong, or Barry Bonds, or Roger Clemmons or Marion Jones. However, what about the rest of the world and our individual and collective drive for improved performance? Here are a few thoughts on the topic and questions for all of us.
Doping With Tylenol?
A number of recent studies show that acetaminophen (Tylenol) can improve cycling performance. This includes repeated sprints, exercise in the heat, and a self-paced time trial:
“Using acetaminophen, participants cycled at a higher mean power output, with an increased heart rate and blood lactate, but without changes in perceived pain or exertion. Consequently, completion time was significantly faster. These findings support the notion that exercise is regulated by pain perception, and increased pain tolerance can improve exercise capacity.”
Is this doping? Should Tylenol be banned? You can tell a similar story and ask the same questions about caffeine.
What About Middle Age?
A recent piece in the Velo News tells the story of a late 50s recreational cyclist with clinical testosterone deficiency who went on testosterone replacement therapy for a number of issues including osteoporosis. The athlete in question self-reported and asked for a therapeutic exemption so he could keep competing in local races. The exemption denied because he did not have a clearly defined endocrine problem. You can also make the case that Viagra like drugs might improve performance in some people especially at altitude. What does this mean for master athletes who take these compounds for other reasons?
For women there is at least some evidence that hormone replacement therapy (HRT) improves exercise capacity but the data are far from clear cut. What about the aging news anchor who uses botox to keep her job?
Is any of this doping when the drugs in question are used for legitimate medical purposes? Search the internet for anti-aging clinics and you will find all sorts of outfits offering unproven (usually hormonal) therapies purported to slow the aging process. Recently, some elite younger athletes have been tweaking their thyroids levels. Where does the “legitimate medical purposes” justification end and doping or snake oil sales begin?
Academic Doping?
For the twenty somethings reading this article the idea of academic doping – using ADHD drugs obtained on the black market to do better on a test is old news. This practice appears to be pervasive on college and even high school campuses. It also appears to be drifting into the rest of the world where decision making and concentration are critical.
There are all sorts of drugs that enhance or might enhance cognition and more are in the pipeline. Who gets them and when is it fair to use them? Is this just another potential edge for the children of the well-off? In a world of high stakes testing for admission to an elite school or academic program should these substances be banned and test takers subject to doping control? The discussion in the cognitive enhancement world mirrors in many ways the sports doping discussion:
“Drugs developed to treat cognitive impairments are proving popular with healthy college students seeking to boost their focus and productivity. Concerned observers have called these practices a form of cheating akin to athletes’ use of steroids, with some proposing testing students’ urine to deter “academic doping.” The ease with which critics analogize the academic enterprise to competitive sport, and the impulse to crack down on students using study drugs, reflect the same social influences and trends that spur demand for these interventions-our hyper-competitive culture, the commodification of education, and our attraction to technological quick-fixes. Rather than focusing on the technologies that are being put to troubling uses, we would be better served reforming the culture that makes these practices attractive.”
Are We All Dopers?
All of us are surrounded by performance enhancing choices beyond the things like the drugs or nutraceuticals we can inject or put in our mouths. The pervasive invasion of technology into almost every aspect of life offers even more opportunities for performance enhancement. In the end, what does it mean to be human in the 21st century:
- What happens when things like Tommy John surgery are used to pre-emptively improve pitching performance before an injury?
- Who draws what lines about what is ethical and fair?
- Should we even strive for a level playing field?
- What does it mean to be a human in a world where almost every imaginable activity might be subject to high tech performance enhancing strategies?
In the end is there any value left in the lone individual struggling against his or her own limits, or is all about return on investment thinking where the individual is just part of a supply chain leading to a more desirable outcome?

LIKE MIKE

SUBSCRIBE TO RSS
