
What is the Purpose of This Workout?
Last weekend I was in Eugene, Oregon participating in a symposium on human performance. A real highlight was listening to 81 year old Dr. Jack Daniels discuss his vast experience training and testing elite runners. This included his reflections and ideas on altitude training and what he learned helping prepare U.S. distance runners for the Mexico City Olympics in 1968. Throughout the talk as he gave examples of what elite runners do, Dr. Daniels kept asking and emphasizing:
“What is the purpose of the workout?”
He commented that if you can’t answer that question then maybe you should rethink what you are doing. As I reflected on this perspective, a number of related questions occurred to me. Here are three to think about:
- What is the purpose of this meeting?
- What is the purpose of this rule, guideline, or metric?
- What is the purpose of this argument?
With my three modifications of the “Daniels’ Question” as a background, I would urge everyone to reflect on their own circumstances and see what modifications you can come up with that might help you navigate your life a little better and more efficiently.

How the USA Got So Fat
You hear a lot of yapping about how the USA got so fat as a nation. All sorts of people want some simple reason for rise in obesity. That having been said, in the next eight charts I want to tell you a little bit about “what we know for sure” and see if I can paint a more complete picture of how this happened.
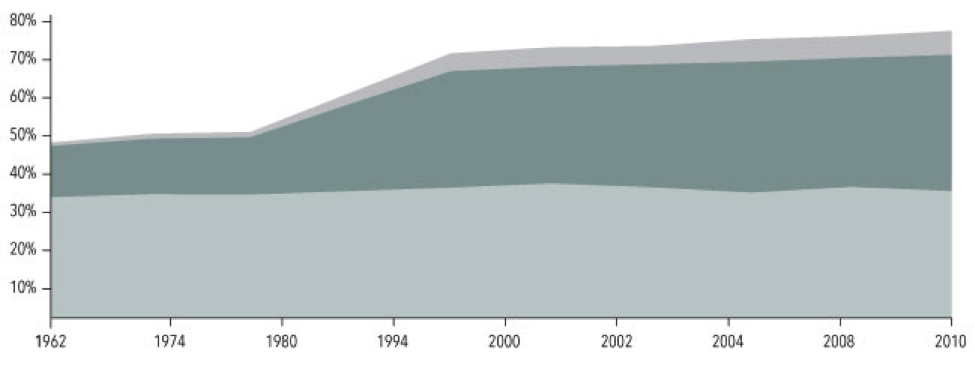
1. Obesity takes off in the late 70s.
The light grey bottom band on this chart from the NIH shows that the fraction of overweight American adults has been pretty constant at about 35% for years. The darker middle band shows that starting in the late 1970s the number of people who are obese has gone from about 10% to about 30%. The top band is the number of people with extreme obesity and it has gone from about 1% to about 6%!
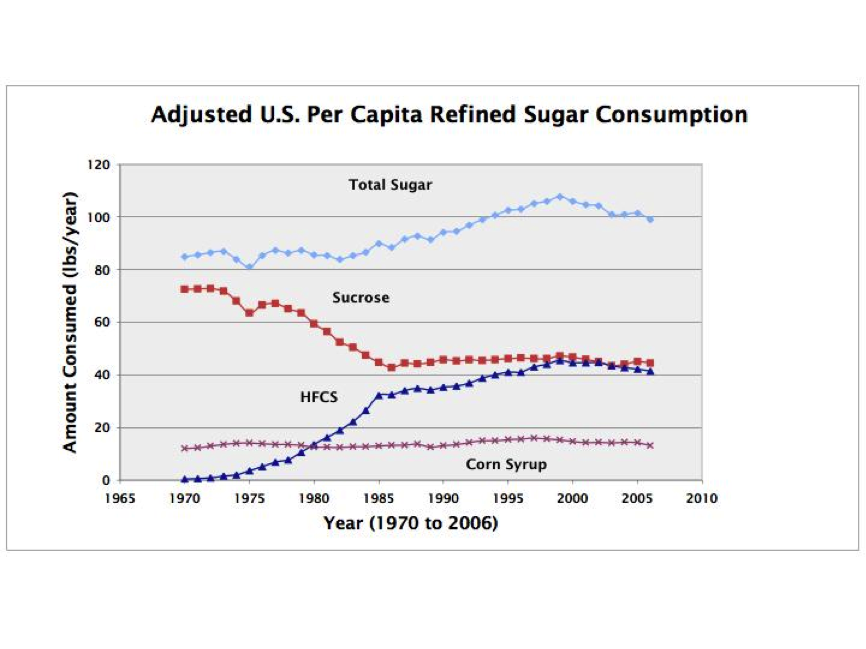
2. Sugar consumption takes off in the early 1980s.
Chart 2 shows that sugar consumption per person has increased from just over 80 pounds per year in 1980 to about 100 pounds per year or more over the last 20 years. Where we get this sugar from has changed too. Sucrose (table sugar) consumption has gone down and High Fructose Corn Sweetener (HFCS) has gone from essentially zero in 1970 to more than 40 pounds per year. This has led some people to label HFCS as the bogyman responsible for “all of this obesity”. A far bigger problem is probably just total sugar consumption.
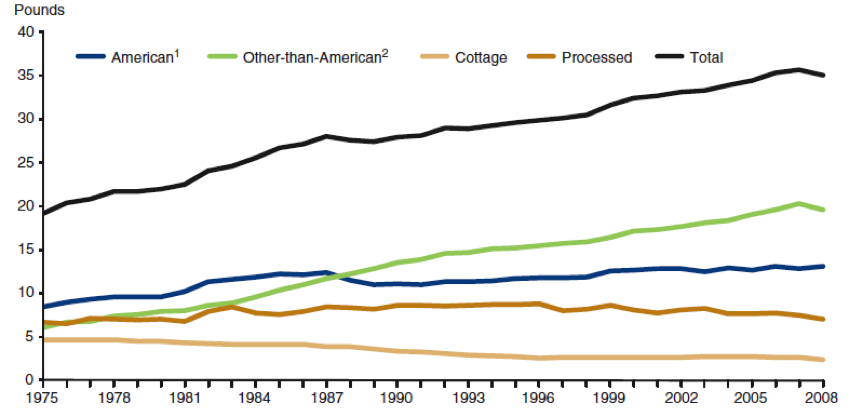
3. Cheese consumption has also skyrocketed.
Total cheese consumption as shown in chart 3 has also gone way up over the last 40 years. I am not sure what this means but just like sugar it is possible to construct a scenario where cheese is the culprit and “cause” of the obesity epidemic. A more plausible explanation is that the sugar and cheese consumption trends show what happens when agriculture policy is designed to generate a lot of tasty high calorie commodities that can then be turned into highly processed and convenient and low cost things to eat.
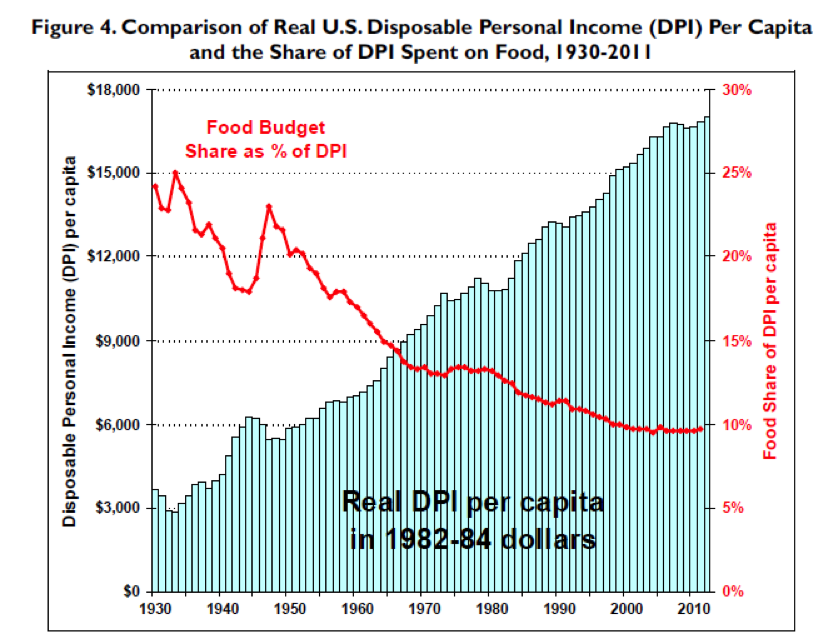
4. Cheap Food?
Chart 4 shows that the average person only spends about 10% of their disposable income on food. That is way down since 1930. The world does not get fat overnight or in just a year or two and the fact that spending on food went down so much in the 1950s and 60s might have set us up for the explosion of obesity that started in the late 70s. As I pointed out in the explanation of chart 3, this is another example of agriculture and food policy contributing to the problem.
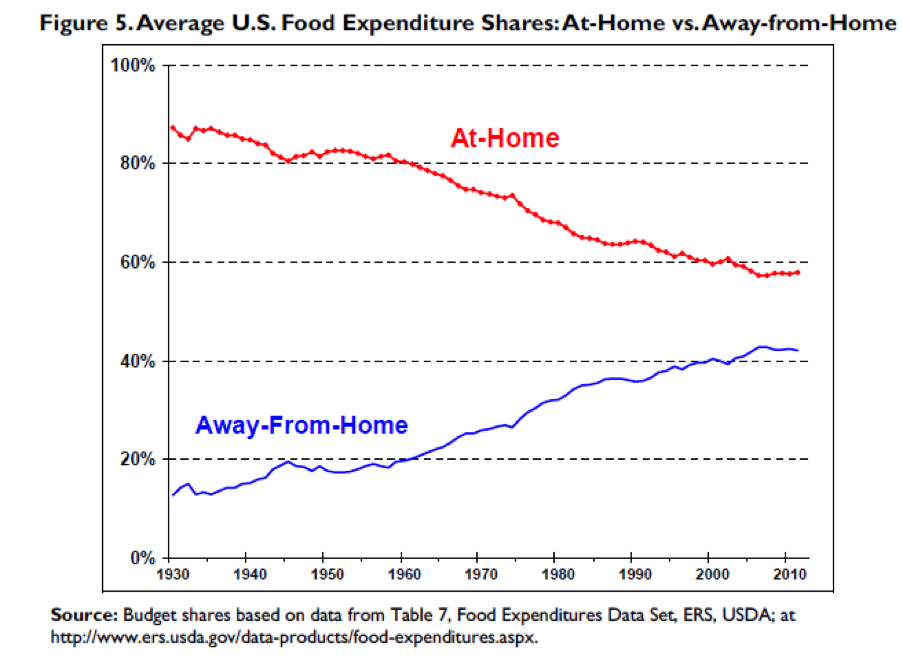
5. Eating Out?
Perhaps another result of “cheap food” ag policy and other changes in society like more mom’s working, people staying single longer, smaller families, and relentless marketing is that we eat far fewer meals at home than we used to as shown in chart 5. The people who sell us this food know how to pack the calories in and pack them in a way that keeps us coming back for more. The average person also typically underestimates the calorie content of the fast food they eat which amplifies the cheap food problem.
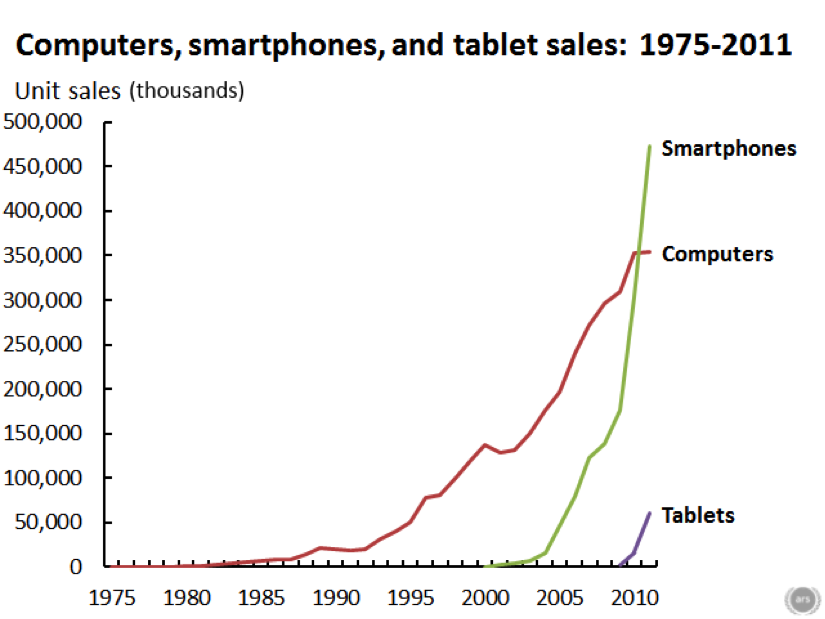
6. Screen time.
Chart 6 speaks for itself and is emblematic of the massive increase in screen time that we have all experienced since about 1980. Sitting in front of a screen can’t be good for your waistline.
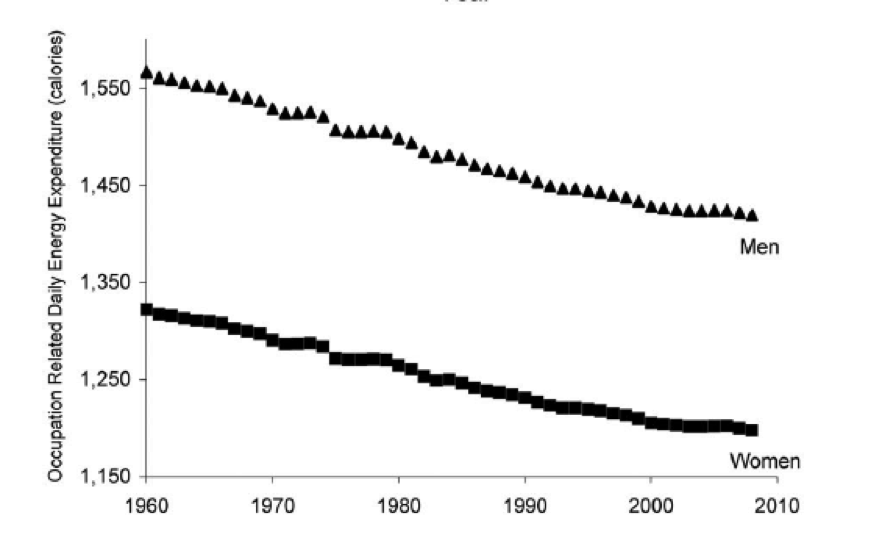
7. Occupational physical activity is way down.
Many people used to work at jobs that required either some or a lot of manual labor. Almost no one doses now, even the mailmen drive. Chart 7 shows that occupational physical activity is down by more than 100 calories per day for both men and women. This coupled with the fact that a lot of people get minimal or no recreational physical activity or exercise is another major problem. Some people have argued that the decline in occupational physical activity might explain most or the entire obesity epidemic.
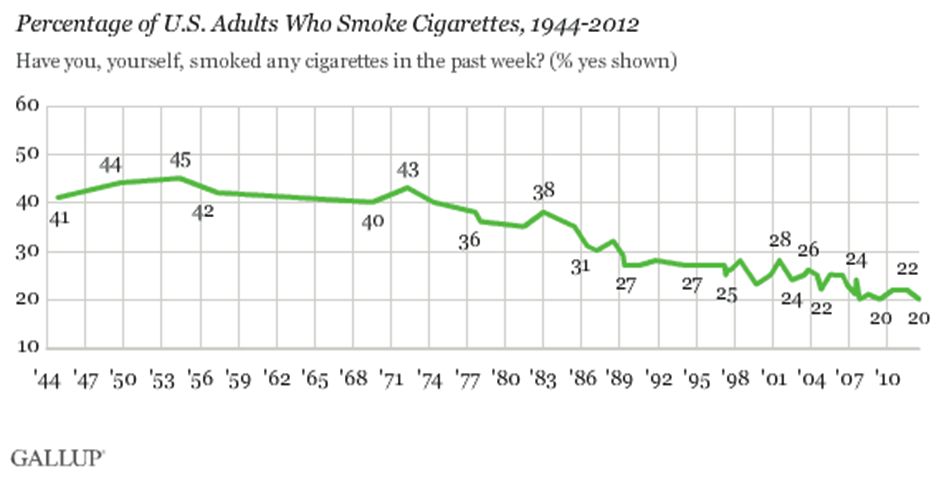
8. Smoking is down.
Smoking has also declined over the last 40 years and smokers tend to weigh less than non-smokers. So, one unintended consequence of the welcome reduction in smoking rates might be more obesity. This is a trade that most public health experts would gladly make except perhaps from people with extreme obesity. Just like sugar and/or cheese consumption, occupational physical activity, and screen time you can argue that less smoking “is responsible” for the obesity epidemic. But as I have tried to emphasize throughout this post, the cause is likely a combination of what we eat and less physical activity and not any “one thing”.
Closing Thoughts
The eight charts above are a sample of the many things that have likely contributed to the obesity epidemic. Thus, it is unlely there is any one explanation for the obesity epidemic and be suspicious of anyone who says there is. The charts also show that a multipronged approach will be required to turn the problem around. Changing food and agriculture policy and what we put in our collective mouths will be one part of any solution. Figuring out ways to get more of the population to build more physcial activity into their day will be the second part.
The “Genetics” of Politics
Earlier this week a piece in the New York Times reviewed some ideas about how “genes” might influence political thinking and explain why people vote the way they do. Like many studies the observations underpinning the assertions about genes and politics rely on comparisons of traits between identical and fraternal twins or perhaps other closely related family members. Since identical twins are genetically identical, the fact that their political attitudes are more similar than fraternal twins is use as evidence that at least some elements of political belief systems are hard wired by genes.
There a number of obvious holes in this argument that parallel those raised in a previous post about genetics of talent. The two most obvious are the shifty definitions of what is a gene and also the inability of people to find discrete snippets of DNA that account for most human characteristics. A great recent example of this problem is from a paper looking at the ability of a large number (more than 60) snippets of DNA to help accurately predict the risk of diabetes. This study found that it is hard to find specific DNA signatures that tell you much about who gets diabetes. We know diabetes is highly heritable, and it is pretty easy to diagnose who is or is not diabetic based on simple clinical tests. However knowledge about DNA does not help much if at all. If we can’t use DNA to predict who is at risk of diabetes, how can we expect to find DNA based explanations for things as complicated as who is at risk for being conservative or liberal?
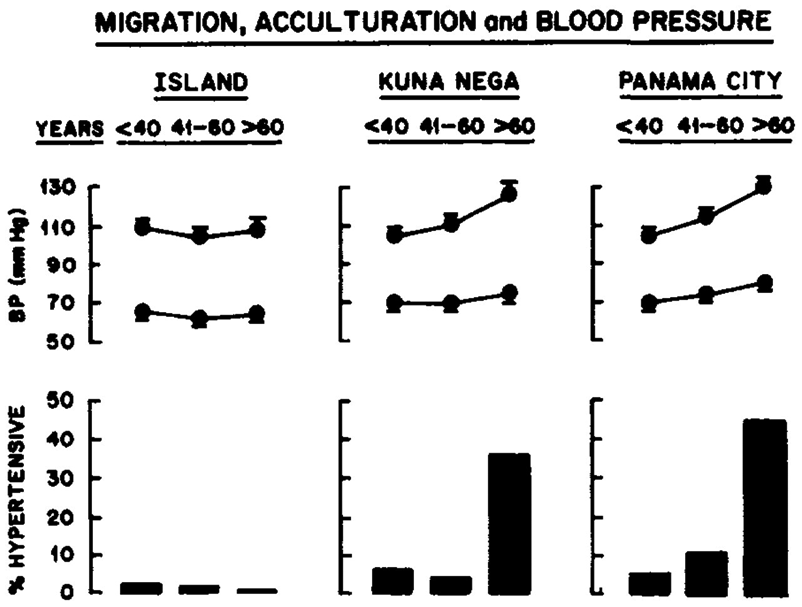
The Environment Matters
Like diabetes a lot of people will tell you that high blood pressure is heritable. However, take a look at the graph below from a study of the Kuna people from Panama. This study shows that depending on where the Kuna live, there are vast differences in the rates of high blood pressure as people age. So, a genetically homogeneous group of people who live in traditional ways on an Island have essentially no high blood pressure, those who live in a tight community (Kuna Nega) in Panama City have a rate of ~30% in those over 60, and the Kuna living all over Panama City have a rate of 40% in those over 60. In the groups living in Panama City there are also more young people with high blood pressure. If you plugged the blood pressure values from people like the Kuna into data analysis programs that estimate heritability and thus the “genetic risk” of various things, you will get wildly different answers depending on the sub population you study.
Whenever Anyone Says “It’s Genetic”…..
The take home message in all of this is that whenever you hear that some complex human trait “is genetic”, remember a few things:
1) The definition of a gene has shifted and many of the ideas about heritability date from the pre DNA definition of what exactly a gene is.
2) For things that are pretty easy to measure like height, weight, blood pressure and diabetes it has been hard to get clear cut DNA signatures that explain much.
3) The environment, behavior and culture matter. A whole lot of thinking about how much of what is heritable depends on the environment and not differences in DNA.
So take assertions about what is genetic with a grain of salt.

{kind=link}
Is Overparenting Soccer’s Grass Ceiling?
The loss by the US to Belgium in the World Cup round of 16 will lead to all sorts of endless speculation about what this means for soccer in the US. As an extremely casual fan who can barely understand why there is not a fixed off-sides line like in ice-hockey, gridiron football, and basketball I think US soccer is a testament to the limits of overparenting. What do I mean?
First, I have been to Brazil and traveled around extensively. In essentially every vacant lot in every neighborhood I saw kids playing pick-up soccer. This was also true in rural areas. Contrast this to the acres of well-manicured fields in suburban America, hyper-organized youth programs, teams named Suburban-United, and minivans galore. The only pick-up games you see are when the immigrant adults show up on Sunday mornings and it is Bosnia vs. Somalia for an hour or two.
Second, drive around “nice” neighborhoods in the US and you see basketball hoops in the drive ways. Have you ever seen a soccer goal? While the NBA is populated by mostly African Americans, it turns out many are not as ghetto as we think. The relentless backyard games played by the Miller family (Reggie and Cheryl) are keys to what made them great players.
Third, all over the country in cities and towns large and small there is “a court” someplace where endless games of pick-up 3 on 3 take place. Everyone interested in becoming a good player knows where this court is and at the better ones you will find a collection of players ranging from solid high-schoolers to people headed to the NBA. Frequently these games have rules like “makers takers”, meaning if you score your team keeps the ball and if your team wins you keep the court. There are no parents, no officials, no fancy uniforms, and no Gatorade on the sidelines. There is also a phenomenon known as “noon-ball” at many YMCAs where in the summer middle aged men give the young guys lessons about holding, hacking, and the finer points of getting an edge. In the parent run world of suburban soccer would this be tolerated? What would happen to Jr’s self-esteem?
Finally, as I watched the US struggle against Belgium to mount attacks I kept asking myself where is the electrifying player who can make it happen? There was no Magic Johnson or Brett Favre to pull it out against long odds the way Lionel Messi did in Argentina’s win over Switzerland in the final minutes. I am also sure that while Magic Johnson and Brett Favre perfected their skills via formal practice, the roots of those skills were developed on playgrounds with no parents around. My bet is that no one drove Magic to the park in a minivan and taught him the no look pass. The paradox of US soccer is maybe that it has to get less organized to get better. Minivans can only go so fast and take you so far.
Big Science: Moonshots or Music?
The announcement in early June that the National Institutes of Health (NIH) was launching a 12 year 4.7 Billion dollar Initiative to study the brain caught my attention and spurred a bit of reflection about the NIH’s last big initiative – the Human Genome Project (HGP). We seem to be in an era of “Moonshot Science” and maybe it is time to ask how the clinical reality of the HGP has done compared to the original moonshot vision promulgated by its many advocates? Have we gotten to the clinical equivalent of the moon?
One of the main ideas behind the HGP was simple: if we know how the DNA based genetic code varies between people with and without certain diseases we will gain insight into the causes of disease. More importantly we can then screen for the genetic variants associated with diseases and offer pre-emptive and preventive interventions to those at greater risk. In some cases we might also be able to tailor drug therapy based on the individual’s genotype. For things like hypertension, heart disease, diabetes, obesity and some cancers this led to what has been termed the common-disease common-variant hypothesis.
At one level the HGP has been a massive test of the common-disease common-variant hypothesis. What are the results so far?
First, for most of the big killers in the developed world mentioned above, clear cut patterns of genetic risk have not emerged. Instead hundreds of genetic risk variants with very small effect sizes have been discovered and the distribution of these risky gene variants is the same in people with and without the disease of interest. Further, when information about these risky gene variants is plugged into risk prediction scoring systems commonly used by Drs, the predictive ability of the scoring systems do not get better. In fact for things like heart disease, diabetes, and hypertension simple knowledge of a patient’s height and waist size tells you far more about disease risk than genetics does.
Second, for common diseases the idea that we could get a gene test and then decide which drug is best for each patient is not working out as neatly as anticipated either. In fact for things like high cholesterol and high blood pressure the guidelines seem to be moving away from the idea that a specific drug might be picked for a specific patient based on genetics. For the commonly used blood thinner Warfarin, which can be tricky to dose, there was hope that information about the genetics of its metabolism would lead to better dosing algorithms, but unfortunately the clinical trials testing this idea failed.
Third, there is increasing evidence that it is difficult for both patients and providers to put information about genetic risk in context. Tell people they are at lower risk and some pay less attention to behavioral factors like diet and exercise that might help them prevent a variety of conditions. Tell them they are at increased risk and at least some get fatalistic and might also pay less attention to behavioral factors like diet and exercise that might help them prevent a variety of conditions. There is also evidence that the perception of increased risk can lead to more tests, biopsies and interventions which all cost money and at least some of them like preemptive surgery have their own set of risks.
Fourth, the HGP seems to have had the “side effect” of encouraging the development of animal models (mostly mice) where an engineered genetic variant leads to a predictable pattern of disease in the animals. This can then lead to the development of drugs that cure disease in animal models but fail clinical trials. One example is Alzheimer’s disease and the idea that it is all about amyloid. A number of anti-amyloid drugs work in the animal models designed to generate a buildup of amyloid in the brain, but twenty plus have failed clinical trials in humans. Additionally, there seems to be a disconnect between the reductionist ideas about amyloid as the cause of Alzheimer’s and the epidemiology data showing the major risk factors for Alzheimer’s include things like diabetes, hypertension, and physical inactivity. In some animal models, the disease of interest does not even show up if the animals are given access to minimal amounts of exercise.
So, based on the issues outlined above I would say some skepticism about moonshot biomedical science including the brain initiative is warranted. This skepticism also seems warranted because so many biomedical breakthroughs seem to be reverse examples of Yogi-Berra’s line about losing by making too many wrong mistakes. In medicine sometimes we win by making the right mistakes. A good example is the drugs that were designed to block the growth of blood vessels in tumors and “cure” cancer. Their effects on cancer have been modest but they have been vision saving in macular degeneration. Likewise drugs like Viagra started out as treatments for heart disease and their effects on erectile dysfunction were an unexpected and profitable surprise for the drug companies. The back story on Viagra is even more interesting because the fundamental observations ultimately responsible for the drug (which led to a Nobel Prize) were the result of a “mistake” made by a lab technician.
In the early 1970s the physiologist Julius Comroe and his anesthesiologist colleague Robert Dripps catalogued the 100 or so key discoveries needed to do then cutting-edge open heart surgery and concluded that about half of them happened by serendipity. Comroe and Dripps questioned the wisdom of too much goal directed big science just at the time the “war on cancer”, an even more dramatic metaphor than moonshot, was starting. As Gina Kolata reported in the Times in 2009, victory in that war is nowhere in sight.
However, there is hope. What the HGP has not revealed along with new ideas from the field evolutionary biology are leading to much more nuanced views of the role that DNA has in influencing the fate of animals including humans. These ideas are showing that DNA is not a simple read only code or program but that it operates in a way that can actually adapt to the environment. My colleague Denis Noble from Oxford has argued that the genetic code is in fact not a code at all but more like a musical keyboard that can be played by other parts of the body and even the environment, behavior and culture. So perhaps we need to stop thinking about biomedical problems as moonshots or wars and more like music. With that mindset maybe we can get to the “right mistakes” generated by all of this big science and find the clinical insights a little bit faster.
Dick Fosbury vs. Guidelines
Over the past couple of years I have argued that the current world wide obsession with “big data” and metrics is going to lead all sorts of people astray in many fields. The related idea is that every human activity can be turned into a quality improvement project with guidelines and check boxes that will reduce error and improve outcomes. Taken too far these twin beliefs are going to limit the sort of individual mastery and innovation needed to find novel solutions to our problems.
A couple of months ago I gave a presentation at Mayo where I highlighted the problems of too much standardization in medicine and the risk it poses to better patient care and innovation. I used parallels with the high jumpers Dick Fosbury and Debbie Brill who as teenagers in the 1960s invented the ‘flop’ and went over the bar backwards. In the current world would their efforts have been stifled by a compliance bureaucracy insisting they face the high jump bar while going over? What would the “approval process” for this new technique be in 2014? How many other barriers might be thrown up in the current world to stop them from moving high jumping forward by going backwards?
I explore these and related issues in the talk below. It is a long presentation about 40 minutes, but bear with me and I think you will enjoy the questions and observations raised in the talk.
How the Heat Lost to the Heat
The big news in the first game of the NBA finals was the air conditioning failure in San Antonio. This surely contributed to Lebron James cramping up and being unable to play the final four minutes of the game as the Spurs pulled away.
As the game wore on, ice packs and cold towels were used in an effort to keep the players cooler, and Lebron apparently changed his uniform at half-time to try to cool down. Might there have been a better strategy to deal with a warm and humid environment with a temperature that was apparently in the 90s at game time? The simple answer is yes.
When our core temperature increases a degree or two, the internal thermostat in our brains activates nerves to sweat gland and we start sweating. The internal thermostat also activates nerves that dilate the blood vessels in our skin and blood flow to our skin increases. If the sweat evaporates the skin stays cool and the blood flowing to the skin cools off. This evaporative cooling system lets the heat generated inside the body get out. When we exercise we produce more heat, and this heat transfer system is even more important.
So, the problems for Lebron and his colleagues included the heat they were producing while playing, the temperature in the building and the reduced ability of their sweat to evaporate due to the humidity. All of this then probably his lead to a viscous cycle of higher body temperatures, more sweating and more skin blood with the extra sweating not helping to cool the body but instead causing more fluid losses. Any extra skin blood flow might also have led to less blood flow for the player’s muscles.
So, what might have been done differently? First, wear less clothing. Any observer of the modern NBA can’t fail to notice the extra clothing and gear a lot of the players are wearing. All of this extra swag creates a microenvironment that makes it harder for the sweat to evaporate and cool the skin. So, if happens again Lebron, ditch the tights. Second, forget the ice and cool towels, they may feel good but if they are too cold they might actually reduce skin blood flow and make core temperature higher. Third, get some fans. The key to the evaporative cooling system I described above is evaporating the sweat. My bet is that there were high capacity fans somewhere in the arena and the best strategy would have been to have players take their shirts off on the bench while the fans created the airflow needed to evaporate their sweat and keep them cool and ultimately in the game.
LIKE MIKE

SUBSCRIBE TO RSS
