
Archive for the ‘Research and Health’ Category
Precision Medicine & Precision Weather: A False Analogy?
One of the ideas riding the wave of enthusiasm for precision medicine is that with enough big data it should be possible to make increasingly accurate “forecasts” about who gets what disease and how it might be prevented, treated or even “cured”. An analogy to precision weather forecasting and climatology is frequently drawn. Cynicism aside about just how good weather forecasting is and how much it has improved, there are a couple of basic intellectual issues with the comparison that are typically glossed over by advocates of the analogy.
Problem 1: The Nature of the Data
Weather data includes things like continuously monitored surface temperature and wind patterns over essentially most of the world. Some of the data is very granular with high spatial and temporal resolution. Things like pressure measurements, above ground temperatures, below ground temperatures, satellite photos, and information on things like humidity are available. There is also a vast store of historical records dating back 100 or more years in many places. This type of multilevel, highly accurate data with essentially continuous time resolution is simply not available even in the most monitored humans living in the real world even with the best monitors. The accuracy of various wearable devices, the granularity of the data, and the historical information they provide pales in comparison to the available weather related data. As someone who has been making some the most detailed possible measurements of human physiology since the late 1970s, things have been miniaturized and made portable, but the quality of the data has not improved and in many ways has gotten sloppier or at least harder to calibrate.
Problem 2: Predicting What?
The other thing to remember is that with weather prediction the goal is to predict what it is going to be like “outside” in a given place on a given day at a given time. Precision weather forecasting does not tell us anything about the temperature and humidity inside “your house” much less inside a given room inside the house. To make that sort of estimate all sorts of additional information is needed about the size of the house, the surface area exposed to the outside world, the heating and cooling system, how insulated the house is, how good the thermostat is etc., etc, etc… Then there is always the possibility that a window is open or that on a cold day you choose to wear a sweater and reduce the temperature “set-point” on the thermostat. The same issues also apply to a given room the house.
The point here is that for human disease, except perhaps for some elements of dermatology, we are generally interested in what is happening inside a specific room inside the body like the “heart” room, or the “liver” room or the “kidney” room. For things like diabetes or high blood pressure that affect multiple rooms, we are interested in the overall house. Also many diseases of specific rooms also frequently do collateral damage to “the rest of the house”. In many of these diseases the ultimate problem that “brings people to the Dr.” has something to do with a complex feedback control system that has gone haywire. That is certainly the case for diabetes, heart failure, and high blood pressure. In heart failure shortness of breath and exercise intolerance is usually the problem patients complain about vs. a weak heart.
So the weather is an outside condition we are trying to predict based on outside data. Medical conditions are generally inside conditions and predicting them from outside data of questionable quality with limited time resolution and historical tracking is clearly an area where the precision medicine vs. precision weather analogy breaks down. Things like biopsies, images and blood tests are inside samples but they are small snap shots and not the sort of continuous measures available to the weather forecasters
Even if we had perfect monitors it remains to be seen if people will actually use them and if the information gained does anything to change their behavior or make them healthier.
Problem 3: What About Inside-out Prediction?
The flip side of the weather analogy is the idea that if you know enough about the building blocks (the cells for example) that make up the house you can predict what is going on inside the house as a whole. Of course the outside world influences what is happening inside and those who favor an inside-out paradigm tend to ignore or discount that problem. Another issue is that unlike static structures humans can move around and change their behavior depending on the conditions outside. When I lived in Arizona I went outside mostly during the cooler parts of the day. In Minnesota where I now live, most of the year, I go outside during the warmer parts of the day. A cell based approach to modeling what is going on inside the body can miss this key but obvious point.
Then there is the problem of the cells as building materials. Imagine decorative concrete blocks like the ones used in the wall shown below.
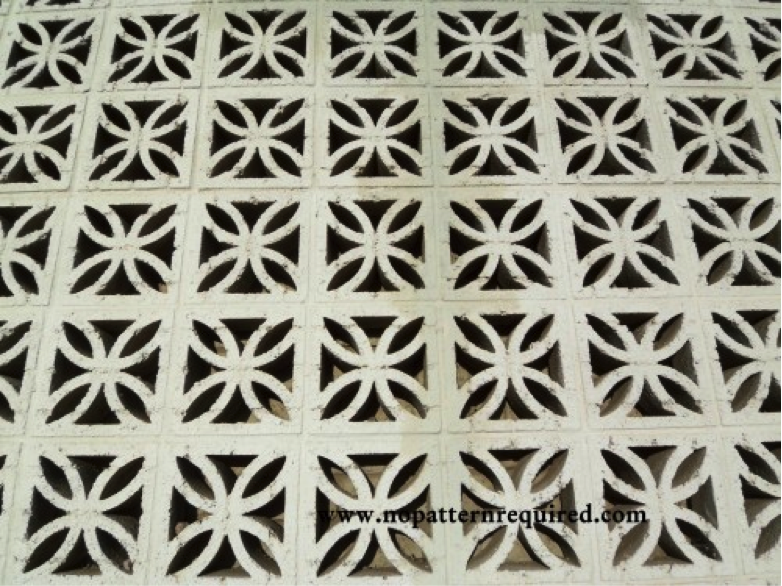
Depending on the orientation of such blocks, a wall made from them can have very different properties. Flip them on their side and a solid vs. porous wall “emerges”. Thus, the temperature inside a structure made from such concrete blocks could vary widely depending on their orientation. However, subject the blocks from a wall of any design to chemical analysis and the “basic” properties of the wall are the same. Things of course get even more complicated if you add a heating and cooling system with a thermostat or other design features that influence the temperature in your concrete block building. This sort of inside-out modeling would be less problematic if the DNA in our cells was a better blueprint for what the “whole building”, but it turns out that DNA is a pretty sloppy and much more adaptive blue print than was once thought.
Closing Comment
I would be curious to see just how much better or accurate weather forecasting has gotten over the years. If there is data on this topic perhaps someone will post a source in the comments section. In the meantime, I hope the concepts noted above make you question the precision medicine, precision weather analogy.

Fitness & Mortality Update
Two recent scientific papers make it time for a quick update on the topic of fitness and mortality.
1. Fitness vs. Cancer Mortality
The first paper is meta-analysis that summarizes the results of a number of studies on the relationship between fitness and cancer mortality. The results were pretty striking:
“Six prospective studies with an overall number of 71 654 individuals and 2002 cases of total cancer mortality were included. The median follow-up time in the studies was 16.4 years. Cardiorespiratory fitness showed a strong, graded, inverse association with total cancer mortality. Using low cardiorespiratory fitness as the reference group, intermediate and high levels of cardiorespiratory fitness were related to statistically significant decreased summary relative risks (RRs) of total cancer mortality of 0.80 [95% confidence interval (CI) 0.67-0.97] and 0.55 (95% CI 0.47-0.65), respectively. Studies that adjusted for adiposity yielded similar results to those that did not adjust for adiposity.”
This means that folks with high cardiorespiratory fitness have about half the risk of death from cancer as people in the low fit group. Usually, in these types of population studies “high fit” is defined as the ability to do “10 mets” of exercise. For example a person with a 10 met exercise capacity can typically run 6 miles (10 km) per hour for few minutes at the end of a maximum exercise test. This is also an exercise capacity that many if not most middle aged people can attain if they watch their weight and workout regularly. So while physical activity and cardiorespiratory fitness are not the same thing, many active middle aged people can get to 10 mets. The flip side of this relationship is that most highly fit people are also pretty active and they do at least some higher intensity exercise training which makes it likely they have a 10 met exercise capacity.
2. Fitness vs. Cardiovascular mortality
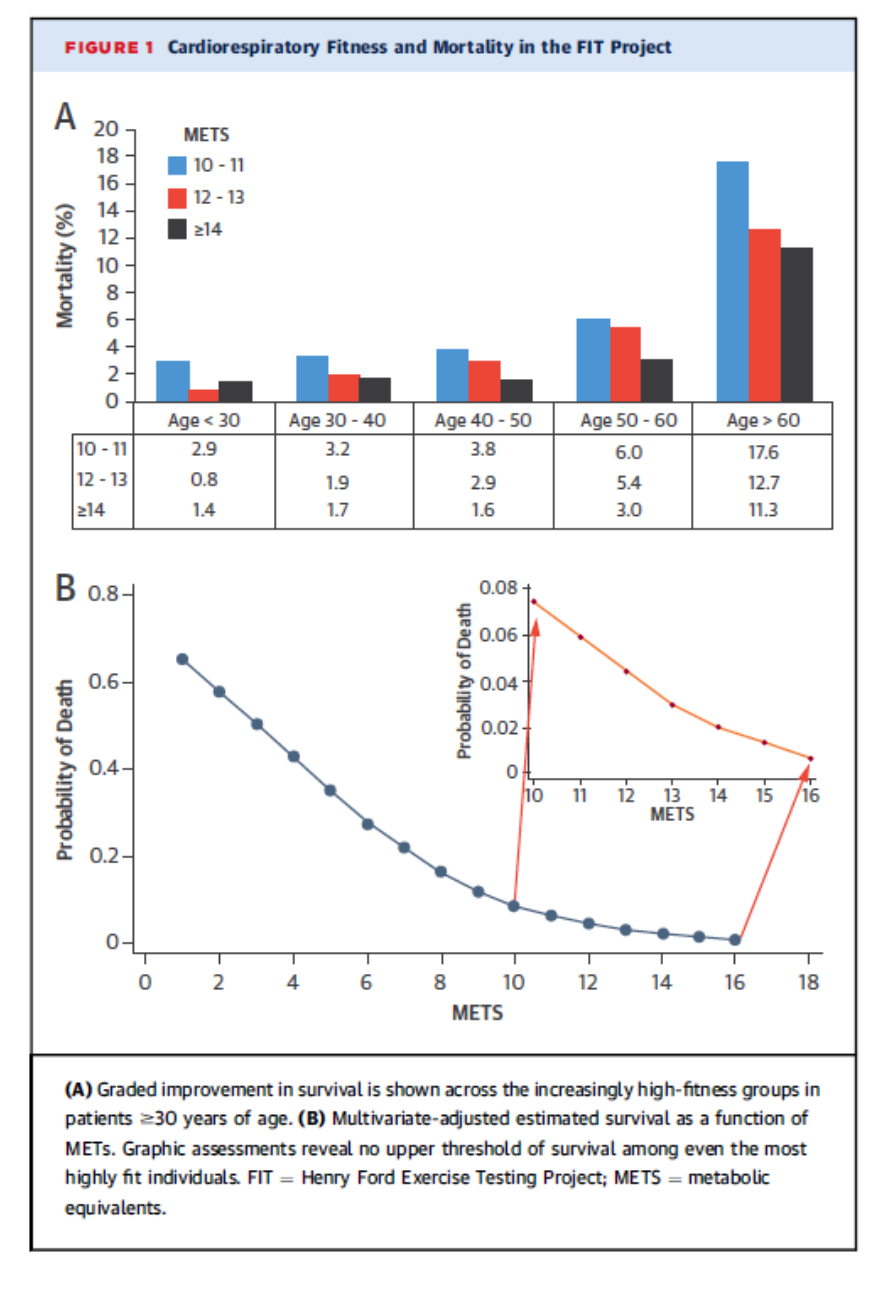
It has been known for a long time that increased fitness is associated with both lower all-cause mortality and lower cardiovascular mortality. A remaining question is whether this relationship flattens out at about 10 mets. In other words do people who can do more than 10 mets have even lower mortality? The graph below comes from a short report on this topic in almost 70,000 people (64% men) followed for about 12 years including about 38,000 with an exercise capacity of greater than 10 mets. The top panel shows that very high fitness was associated with lower mortality in all age groups. The bottom panel shows the dose response relationships between fitness for the entire study population. So greater fitness equals lower mortality.
Summary
Evidence for the protective effects of fitness and its close relative physical activity keeps piling up. The cancer data is especially heartening, and that fact that things don’t flatten out for fitness vs. mortality at very high levels of fitness is perhaps another piece of objective evidence against the too much exercise “hypothesis”.
Moonshots & Medicine
Yesterday I was fortunate enough to land a featured op-ed in the New York Times about precision medicine in specific and the general topic of moonshots in medicine like the war on cancer. For those interested in learning more about these topics here is link to a classic paper by Comroe and Dripps on medical innovation and goal directed progress via “big science” vs. blind luck and marginal gains leading to progress. On a related note Bill Gates recently reviewed the 10 year results of his billion dollars of spending to improve health in the developing world. His conclusion was that not much had changed……
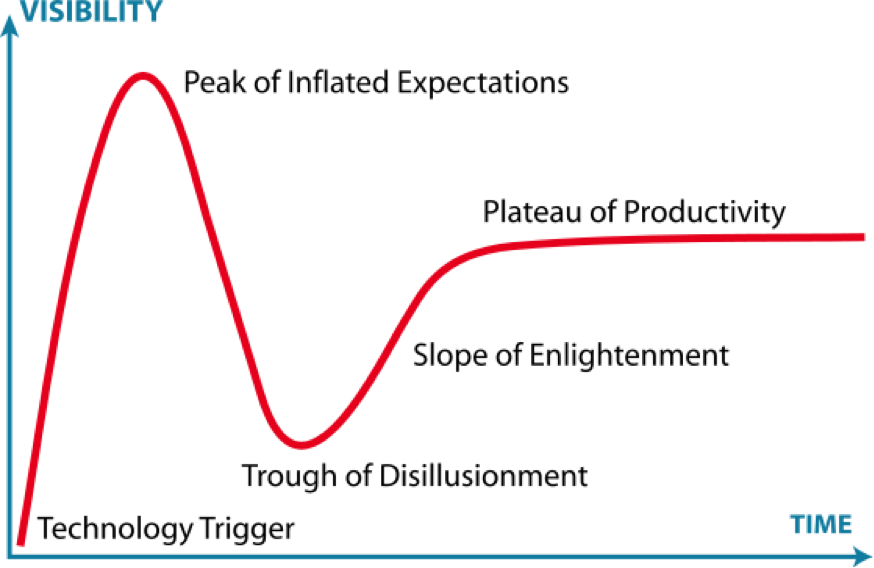
The graphic below is about the hype cycle. The question is always when and how long does it take to hit the plateau of productivity and just how high is it compared to the original expectations.

Remarkable Old People: Share Your Story!
Over the Holidays I bumped into a colleague who told me about her 95 year old father (a retired pharmacist) who is still physically active and living independently. He walks two miles per day, and plays golf (he shot his age at 91, but is now “only” doing 9 holes). He is also active in his church and community. The other interesting thing is that “Dad” had a hard time retiring and for many years pinch hit in pharmacies in the upper Midwest that were short staffed. My colleague also mentioned in follow-up e-mails that her Dad lost his mother in childbirth, was a WW2 veteran who got off the farm and into the pharmacy via the GI Bill, and he also quit smoking back in the 1960s.
Did He “Know” Lester Breslow?
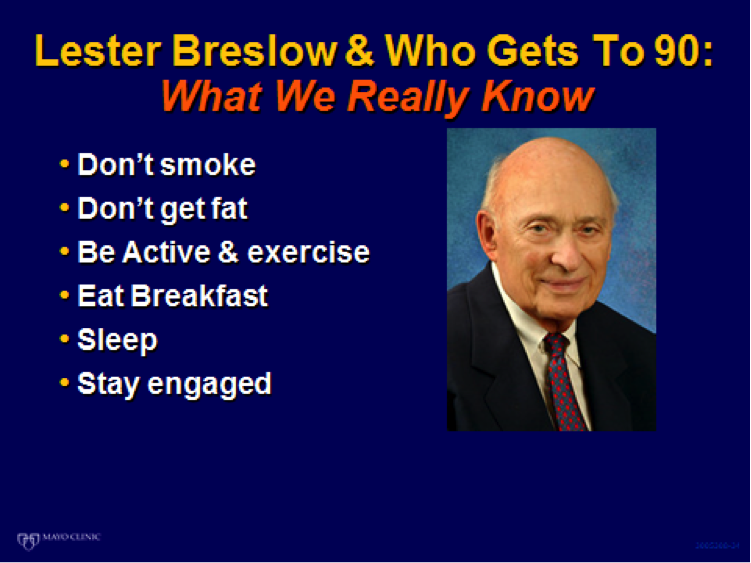
The graphic below is one I use in talks on healthy aging and “who makes it to 90”. It highlights the key principles on this topic that were discovered by the pioneering epidemiologist Lester Breslow. When I heard the story of my colleague’s father what Breslow discovered certainly seems to ring true for “Dad”.
Circumstances & How You Respond
The other thing that hit me about “Dad” in specific and that also seems to apply to many healthy agers is how resolute and resilient they have been over the years. Somehow they all seem to understand — or maybe have learned — that you can’t always control the circumstances you find yourself in but you can control how you respond. At some level this may be a learnable life skill and the Holocaust survivor and famed psychiatrist Viktor Frankl felt that resilience can be learned. He noted:
“Forces beyond your control can take away everything you possess except one thing, your freedom to choose how you will respond to the situation.”
Please Share Your Story
I personally find stories like the one above to be incredibly interesting and inspiring. If you have one, please share it in the comments section and in a future post I will highlight the key messages and insights.
Thanks and remember the words of John Wooden:
“Do not permit what you cannot do interfere with what you can do.”
New Year’s 2015: Drinking Charts to Ponder
Who can think about New Year’s without thinking about drinking. The chart below is about 15 years old but still considered accurate and shows the relationship between drinking and the risk of cardiovascular disease. It shows that moderate alcohol consumption (essentially 1-2 standard drinks per day) is generally protective.
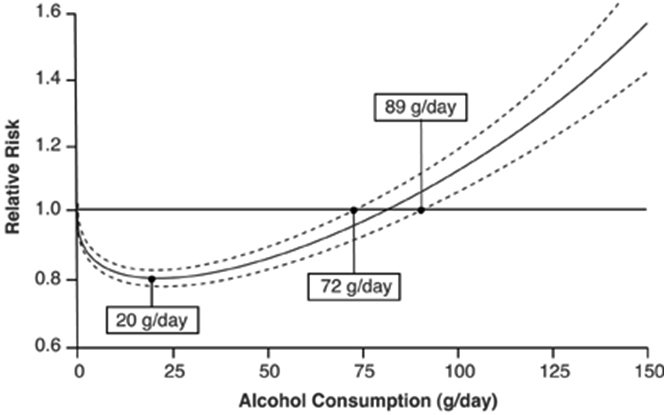
While moderate drinking is generally good for you, it is important to remember that binge drinking (4 drinks for women 5 for men) is bad news, and it is common.
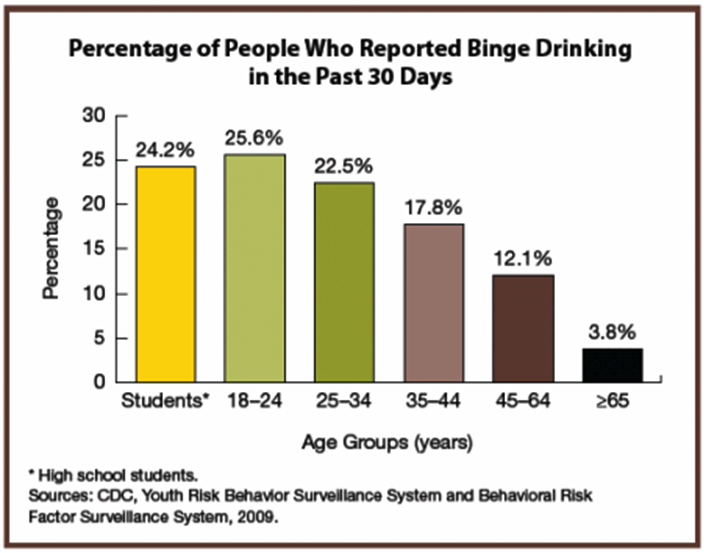
The highlights of the bad news according to the CDC include:
- Motor vehicle crashes. Every day, 32 people in the United States die in motor vehicle crashes that involve an alcohol-impaired driver.
- Intimate partner violence. About 2 of 3 incidents of intimate partner violence are associated with alcohol.
- Risky sexual behaviors. Excessive drinking increases risky sexual behaviors, including unprotected sex and sex with multiple partners, which can result in HIV infection, other sexually transmitted diseases, and unplanned pregnancy.
- Fetal alcohol spectrum disorders. Any alcohol use by a pregnant woman can cause harm to a developing fetus, resulting in physical, behavioral, and learning problems later in life.
- Chronic conditions. Over time, excessive drinking can lead to alcohol dependence, liver disease, high blood pressure, heart attack, stroke, and certain kinds of cancer.
Summary
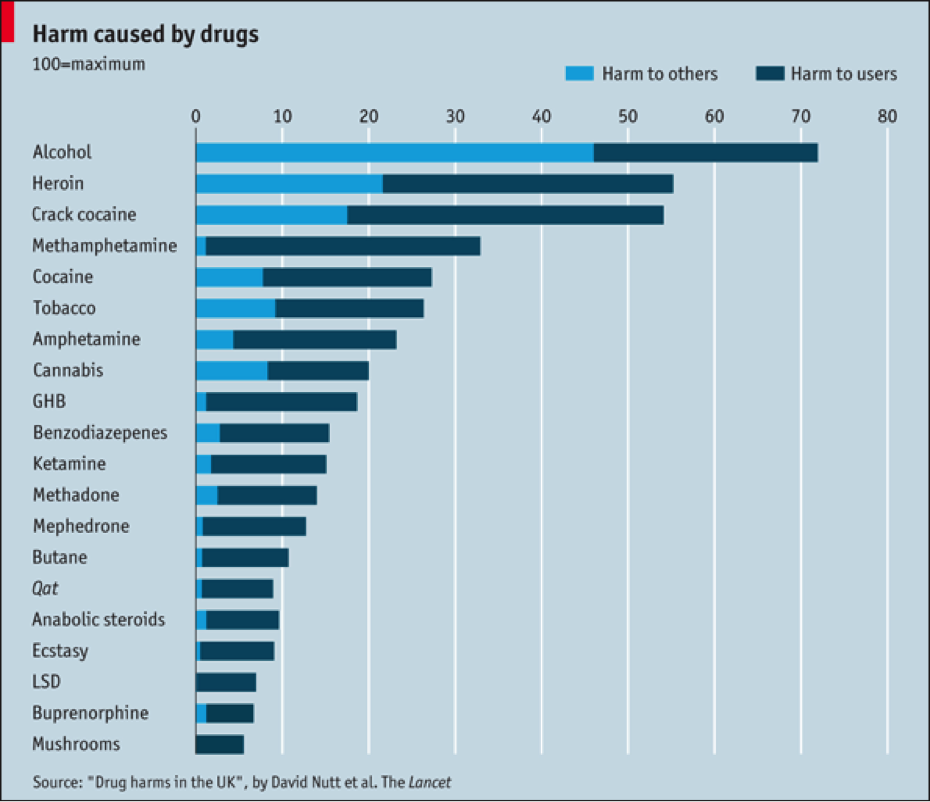
The data above and resources in the links speak for themselves. Enjoy New Year’s and every other social occasion that includes alcohol but remember that alcohol is perhaps the most dangerous drug and needs to be used judiciously.
Obesity and Bargaining
A couple of weeks ago I floated the idea that for many problems facing the world a sort of collective grieving process is going on. In this post I want to pick up on that theme again as it applies to obesity. In general, for obesity I believe we have mostly moved beyond denial and are now “bargaining” about what to do about obesity both as individuals and society as a whole.
Costs of Obesity
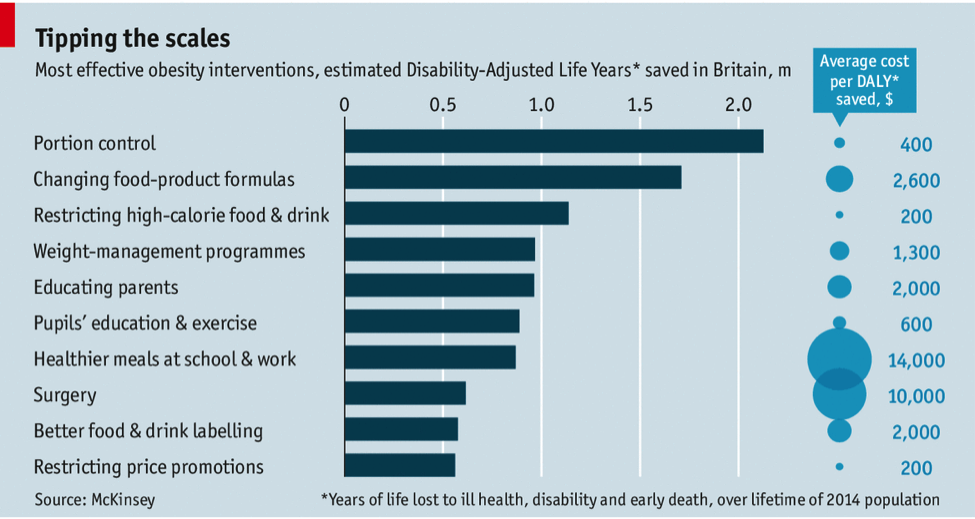
Last week the big consulting firm McKinsey released a report on the global costs and consequences of obesity and what to do about it. Incredibly the report put the global costs of obesity at about 2 trillion dollars per year. This is about equal to the global costs of smoking and also the global costs of “armed violence, war and terrorism”. The report concluded that no single action is likely to solve the problem but that a range of policy options might work. The chart below is an example of what various anti-obesity interventions might do to obesity related years of life lost in Britain. My guess is that similar calculations would also apply to the U.S. and most countries where obesity is a serious problem. Of note I see at least three things missing from this chart:
- Taxes on high calorie foods or sugar sweetened beverages
- Higher insurance premiums for obese individuals
- Re-engineering the built environment
Denial Not Gone
At the same time the McKinsey report was coming out, the U.S. CDC was being pressured to take down a website called “lean works” that included an obesity “cost calculator”. The concern was that such a tool might lead to workplace discrimination against obese individuals. So, perhaps denial that obesity is a problem and that something needs to be done about it is not totally gone.
Who Stays Lean?
Last month I was giving a talk in Denmark about what to do about physical inactivity and obesity. The talk was to a group of health care professionals who were uniformly lean and fit. Being Danes, many ride their bikes to work. So, at some level I was preaching to the converted. What occurred to me as well during the talk was that I was also talking to a group of highly educated people who all had a suite of behavioral characteristics that let them control their current behavior to prevent a future undesired outcome. In other words these people all had a sense of delayed gratification and conscientiousness. These traits likely permitted them to adopt and adhere to “healthy” lifestyles and remain lean in an obesogenic world. From what I can tell only a modest fraction of the population has a high level of these behavioral traits and skills. So what do we do in a world where so many people have so much trouble with what might be described as “self-control” and personal responsibility?
Beyond Personal Responsibility?
This brings me to the built environment and other big picture interventions to address the obesity and inactivity problem. The next chart shows how the battle against infectious disease was largely “won”. A lot of this had to do with things like sewers and clean water supplies. In other words, basic sanitation and civil engineering vs. medical care or medical interventions made a big difference.
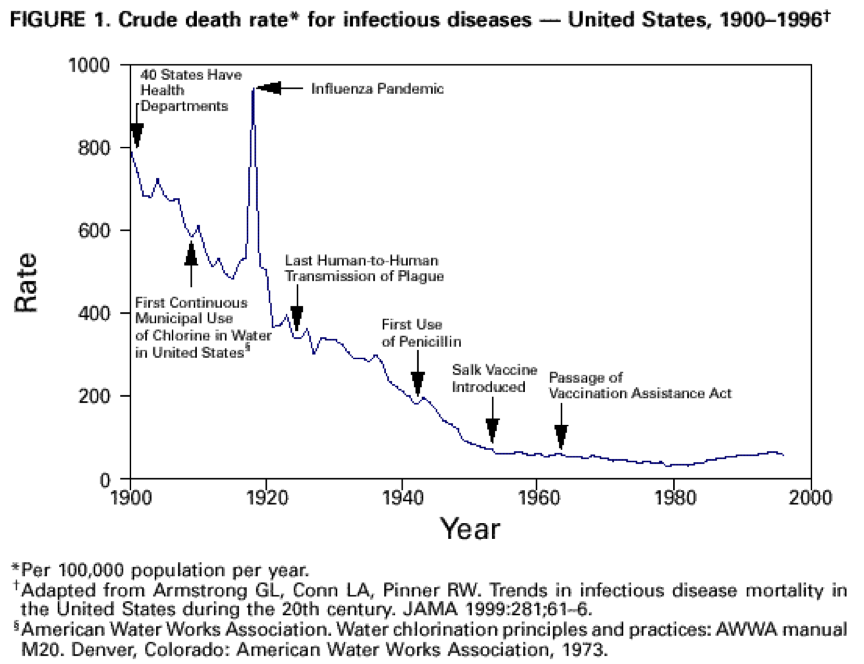
When big, dirty and disease ridden cities were being re-engineered and rebuilt in the 1800s and early 1900s, no one was telling the general public that clean water was their “personal responsibility”. Instead slums were cleared and sewers and water works were built and things like cholera epidemics stopped. That having been said, I wonder how many people in today’s world would consistently boil their own water over days, months, and years in the absence of reliable clean water supplies. My guess is that over time only the most conscientious people would do it. At some level our current world is just as toxic and maybe larger scale interventions are needed.
Going Far Enough?
I applaud the McKinsey report, but does it go far enough? My guess is that many of the food policy recommendations will likely work if they can ever be implemented in a comprehensive way. However, I also have serious doubts about whether that can be done. I also believe (as cigarette taxes have shown) that humans are price sensitive and that economic tools have to be part of the solution to the obesity problem. There also probably needs to be a serious discussion about how car “unfriendly” the world needs to be if we really want to make a dent in the inactivity element of the obesity epidemic. It is hard to imagine that our physical world might be redesigned in a way similar to what happened in cities 150 years ago, but perhaps it will happen. There are innovative proposals on the table in London to promote more bikes and fewer cars.
None of this will be easy, but the partial success of the anti-smoking movement in some countries shows that over time it is possible to change bad societal habits, but it takes more than simple personal responsibility. So let the bargaining begin!
You are currently browsing the archives for the Research and Health category.
LIKE MIKE

SUBSCRIBE TO RSS
