
Archive for the ‘Health Policy’ Category
Bait & Switch: Longevity and the Medicare Eligibility Age
In a post last week I reviewed data on life expectancy and implications for the retirement age especially in the context of proposed changes in the eligibility of Medicare. Here is a link to a retirement age calculator for the U.S. Social Security system. For those born after 1938 the age gradually increases to 67 for those born in 1959. The retirement age for Medicare is currently 65, but up for discussion in the ongoing debates about the fiscal future of the U.S.
The idea driving the Medicare debate is that people are living far longer than they were when the program was started and thus an upward adjustment is needed to make Medicare demographically realistic and limit the explosive (and unsustainable) increases in costs for this program as the baby boomers retire. Opponents of this idea point out gains in life expectancy have been uneven and that most of the gains have been in relatively well-off segments of the population. There are also significant life expectancy differences based on race, education and sex (women live longer). Thus, the idea is that raising the retirement age would be “unfair” to certain groups. As I pointed out last time, no one ever brings up the general “unfairness” of these programs to men which I find a bit puzzling but will leave to the pundits to sort out.
The counter argument about the potential unfairness of raising the eligibility age for Medicare is that the real problem is what happens to or in the groups with lower life expectancy before age 65. In other words, the differences in life expectancy in various subgroups for those who make it to 65 or older in pretty good health are less dramatic than the differences in life expectancy from birth data would suggest. What follows are some examples of what happens to people before age 65 that might explain some of the socioeconomic differences in life expectancy.
Physical Activity
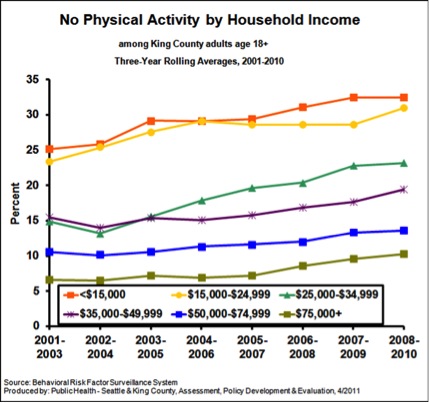
The figure below is from King County, Washington (Seattle) and shows data on the influence of income on “no physical activity in the last month”. As I have pointed out repeatedly, physical activity is extremely protective against all sorts of problems and increases longevity dramatically.
Obesity
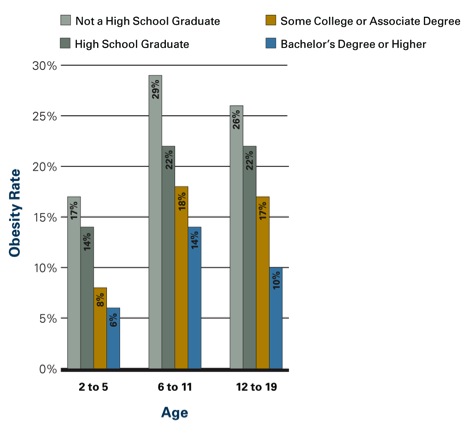
The figure below shows the influence of parental education on obesity rates in kids. Similar data is available for adults. In adult women those with more education and higher incomes are less likely to be obese. In men the relationship is not as clear, but there is some evidence that better educated men are less obese the less educated men. However, the bad news is that obesity has increased for both sexes and all socioeconomic and racial subgroups in the last 20 plus years.
Smoking
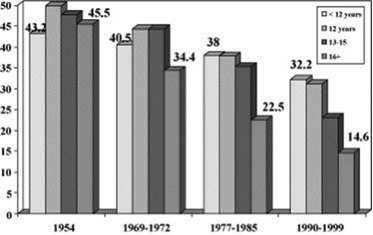
The figure below shows data on smoking rates by education (usually a close correlate of income) and how they have changed between 1954 and the 1990s. Rates have fallen for all groups but most dramatically for the most educated people.
Social Stress
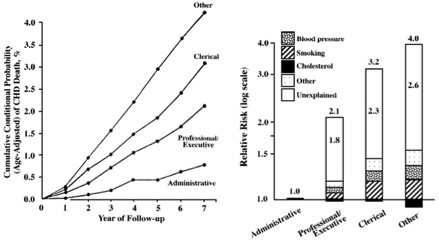
There is pretty good evidence that social status and what might be described as social stress and autonomy plays a role in the early mortality seen in less educated and lower socioeconomic status groups. In other words, poor and less educated people have less control over their daily lives and that is stressful and bad for their health. Social stress is also independent of traditional risk factors or access to care. The figure below shows how job category/education affects cardiovascular mortality in civil servants in England. The bar graph on the right of the figure is a “log-scale” so a bit distorted, but the overall picture is clear. The article points out that:
The cardiovascular mortality rate over 7 years in 17 530 London civil servants was more than 4% among unskilled workers, compared with 3% among clerical workers, 2% among professionals or executives, and less than 1% among administrators. The presence of identified risk factors, including cholesterol level, blood pressure, and smoking, explained less than half of these differences. All of these persons were working at the onset of the observation period and had access to medical care through the National Health Service. Therefore, neither biomedical risk factors nor limited access to medical care can account for most of the differences, and the major component of differences in the risk for cardiovascular death remains. We suggest an explanation based on lifestyle and behavioral considerations.
My bet is that the more educated and higher paid civil servants in the UK were much more likely to be physically active, watch their diets and otherwise comply with health guidelines and medical advice.
Summary
All sorts of issues including physical inactivity, obesity, smoking and social status/stress need to be addressed to reduce the effects of socioeconomic status, education and race on life expectancy. However, most or all of these issues need to be addressed prior to the age of 65 to have much of an effect on life expectancy. Most are also relatively independent of access to medical care. Confusing these issues, with the eligibility age for and long term finances of Medicare is an example of a policy discussion bait and switch.

Longevity and the Retirement Age
Much of the long term pressure on the finances of the Federal Government is being driven by rising expenditures on health care and pensions and much of this is being driven in turn by an aging population. This has led to proposals to raise the retirement age especially for Medicare. You will likely be hearing more about the retirement age as our political “leaders” try to figure out what to do next in terms of taxes and spending.
Here is a proposal from the conservative Heritage Foundation on this topic, but they are not alone and many “centrist” groups are proposing increases in the retirement age for Medicare. This idea has been criticized by people like the economist turned political commentator Paul Krugman as unfair because the increases in overall longevity in the U.S. have been uneven and not shared by all socioeconomic and racial subgroups in the country. Today I want to take a deeper data driven dive into this topic.
1. The big picture. In an earlier post on longevity I pointed out that in 1960 about 60% of men and 71% of women lived to age 65. The men who made it to 65 then lived an average of about 13 years and the women who made it to 65 lived another 17 years. In 2010 about 84% of men and 89% of women made it to 65. The average man who makes it to 65 now lives another 16-17 years and for women it is about 19 years. These changes are being amplified by the fact that the leading edge of the baby boom generation is reaching retirement age causing a further bulge in the aging population. You don’t have to be a rocket scientist to realize these demographic trends are putting pressure on Federal finances.
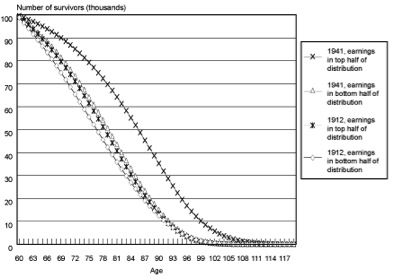
2. Differential Increases in Longevity and Socioeconomic Status. I mentioned above that critics of the idea of raising the retirement age for Medicare point out that most of the gains in longevity have been in people that are relatively well off. The graph below is from a study by the Social Security Administration and shows survival curves starting at age 60 for men comparing those born in 1912 with those born in the 1941. The key observations are that: a)in 1912 there was not much difference in life expectancy between the top and bottom half of income distribution, b) the bottom half of the 1941 cohort does not look that different than either group from 1912, and c) that life expectancy at age 60 has really gone up for the better off men born in 1941. There are lots of ways to slice and dice data like this but pretty much every way you do it comes out the same and gains in life expectancy have been greater for people who are better off.
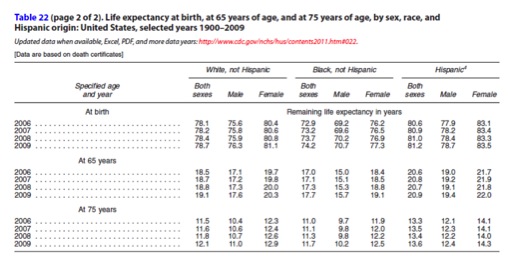
3) The race and education snapshot. Below are a table and graph from summary data from the U.S. Centers for Disease Control in 2011. The table shows life expectancy at birth, 65, and 75 in recent years. What is interesting here is that the differences in life expectancy between Blacks and Whites at 65 and especially 75 are much lower than the projected differences at birth. The other interesting thing to note is that Hispanics are higher than either Blacks or Whites in all of the major comparisons. I interpret this in a couple of ways. First, a big issue here is not what happens once people reach the standard retirement age of 65, but what is happening prior to age 65 especially in Blacks. The other issue here is that women do better than men and I have not heard any of commentators claim that raising the retirement is unfair to men.
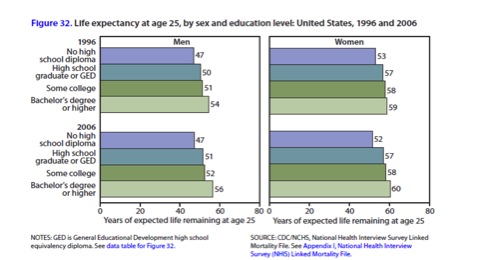
The next figure shows life expectancy at age 25 in 1996 and 2006 by education level and sex. This table shows a couple of things including: a) educated people live longer and there is a dose response curve, and b) life expectancy at age 25 for less educated people has stagnated. This figure also shows that women live longer than men at every level of education.
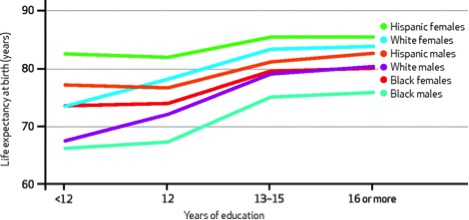
4) A summary slide. The figure below is a summary slide that shows the effects of race, sex, and education on life expectancy at birth. These differences would likely exist at age 65 but be much smaller in terms of absolute years. The article this figure was taken from indicates that some of these differences might be getting worse.
My take on all of this data. There are all sorts of ways this data can be analyzed. For the purposes of thinking about the retirement age a couple of things stand out.
- People as a whole are living longer but the gains have been uneven and influenced by sex, education, and race. There are also probably pretty tight relationships between race, economic well-being and education.
- A lot of the problem is not about what happens when people reach age 65, but what happens before age 65. People with lower socioeconomic status tend to have a host of behavior and risk factor issues that negatively influence their ability to make it to 65 and then do as well after age 65. So the real issue here is how to address health disparities vs. the fairness of raising the retirement age.
- Many of the factors leading to health disparities like differential smoking rates, obesity, lack of physical activity, and violence have little to do with what we think of as traditional health care and will not be fixed if and when high quality health care is available to all.
- There is also an argument that people are retiring too early for economic reasons and that a lot of people are financially unprepared for the long life they are likely to live in retirement. If raising the eligibility age for Medicare encourages people to work longer, maybe that is good for their own long term economic well-being as well as that of the country as a whole.
Closing comments. The discussion about the fairness of raising the retirement age for Medicare has been marked by incomplete thinking about the data and is confusing the very real problem of what to do about health disparities based on race, education, and sex with the arithmetic of Federal finances. Some of this discussion is being led by people with overtly political and personal agendas like Paul Krugman (who should know better) at the expense of a hard look at the facts.
Health Care Costs and Physical Activity
Today’s post is brief and shows data on health care costs and physical activity in Medicare patients from about 10 years ago.

The figure shows average annual total health care costs for adults over age 65 who had either worked for General Motors or were spouses of former GM employees. The subgroups in the figure are based on body mass index (a marker of obesity) and also those who were inactive (0/wk), active 1-3 times per week and active more than 4 times per week. Over 40,000 people were involved in the study. For each body mass index subgroup, health care costs were lower and there seemed to be a dose response effect. In other words the most active people had lower costs than the moderately active people who had lower costs than the least active people.
While this data is interesting and certainly suggests that more activity equals lower health care costs, there are limitations. For example, perhaps the most active people were simply healthier to begin with and as a result could be more active. In future posts I will explore what is known about the effects of interventions that promote physical activity on overall population health and also health care spending.
More Thoughts About Taxing Unhealthy Behavior
Depending on who you believe any long term solution to the fiscal issues confronting the United States will include revenue increases of 800 billion to 1.6 trillion dollars over the next 10 years. From what I can tell almost all of the discussion about how to raise that revenue focuses on what the well-off will pay. Will their income tax rates be higher, will their deductions be lower, and will the tax code be revamped so that things like capital gains are taxed at a higher rate? As someone interested in public health it seems to me that the revenue, and more importantly behavioral changes, associated with sin taxes should be considered in this debate.
- The Congressional Budget Office estimates that nearly 80 billion dollars could be generated over the next 10 years by increasing the tobacco tax by about 50 cents per pack.
- Obesity researchers and economists from Yale and the University of Illinois Chicago have modeled the effects of a 1 cent per ounce tax on sugary beverages and estimated that nearly 20 billion dollars per year could be generated (200 billion over 10 years).
- The alcohol tax as a percentage of the total cost of various forms of alcoholic beverages is much lower than it was in 1980. If the alcohol tax was 30% of the pretax value of the beverage (it is currently about 10%), a study by the Cato institute estimated that federal revenues would increase by 25 billion dollars per year (250 billion over 10 years)
- Demark recently repealed their so-called fat tax. It was generating about 200 million per year in taxes on high fat foods for the Danes. Extrapolate that to the U.S. which has about 60 times the population of Denmark and you get about 12 billion in revenue per year or 120 billion over 10 years.
All of this adds up to about 650 billion dollars of increased revenue over ten years. Additionally, there is pretty good evidence that smoking rates, health problems associated with excessive drinking, and perhaps even obesity rates might fall if these taxes were enacted. For example a 10% rise in cigarette prices typically reduces consumption by 4%. The sugary beverage tax is estimated to reduce consumption by about 24%, and the alcohol tax is estimated to reduce consumption on the order of 10%. These behavioral changes would likely have positive effects on health care spending over time. There are also economic arguments about improved productivity and increased spending in other parts of the economy that would flow from things like less smoking and drinking.
One of the major arguments against sin taxes is that they fall disproportionately on the poor. However, the counter argument is that the positive behavioral changes associated with these taxes would probably disproportionately benefit the poor in terms of improved health over time and more money to spend on other things. This is especially important because policies that promote positive behavioral health changes in the poor have been difficult to implement and results have been marginal in many cases.
The figure below is from an article on health disparities in 8 socioeconomic groups in the U.S. and shows the role of common behavioral factors in disease burden (for the record I would argue that they grossly underestimated the effects of physical inactivity). These factors are typically higher in the socioeconomic and racial groups with the worst overall health and lowest life expectancy. Increased taxes on tobacco, alcohol and foods contributing to obesity would clearly help reduce the burden from the top four or five causes.

As the article notes:
“Disparities in mortality across the eight Americas, each consisting of millions or tens of millions of Americans, are enormous by all international standards. The observed disparities in life expectancy cannot be explained by race, income, or basic health-care access and utilization alone. Because policies aimed at reducing fundamental socioeconomic inequalities are currently practically absent in the US, health disparities will have to be at least partly addressed through public health strategies that reduce risk factors for chronic diseases and injuries.”
That having been said, I would argue that sin taxes should be attractive to liberals concerned about racial and socioeconomic disparities for statistics like life expectancy and other measures of overall health.
Sin taxes should also be attractive to conservatives who typically espouse a preference for policies that promote personal responsibility. Sin taxes would also help address the current conservative narrative about makers and takers because the increased taxes would tend to fall hardest on states that receive excess federal funds relative to the taxes they pay…..what might be described as “taker” states.
The changes in tax policy that will be made in the coming years have the chance to make things fairer, simpler, more transparent, and perhaps spur economic growth. The ideas outlined above have the added advantage of improving public health, raising revenue, and perhaps driving health care costs down in the longer run. Sin taxes also have the opportunity to address both liberal and conservative policy goals, so shouldn’t they be part of any solution designed to put our financial house in order?
Taxing Unhealthy Behaviors?
There has been a lot of discussion about things like soda taxes to reduce unhealthy behaviors and address the obesity and diabetes epidemic. The idea is that as prices rise, sugary drink consumption will fall and this will have an impact on obesity and diabetes and ultimately reduce some of the upward pressure on health care costs. Along these lines, Denmark implemented a “fat tax” for high fat food items a few years ago but recently reversed the tax for a number of reasons. Importantly, the fat tax in Denmark was not around long enough to determine if it would have any impact on public health. By contrast it is pretty clear that cigarette taxes have contributed to reductions in smoking rates.
Another idea out there is to ask people to pay differing health insurance premiums for what might be called “behavioral” risk factors that are subject to personal choice and changes in behavior. For example, smokers would pay more for their health insurance than non-smokers. The question is how far to take this approach. In some insurance plans there is a move to charge people more for obesity, high cholesterol, hypertension, and diabetes (this would be in addition to higher charges for smokers). The plan would then lower rates or offer rebates as people with “controllable” risk factors addressed their issues and got “their numbers” under control. In other words, if they lost weight, took their blood pressure, cholesterol and/or diabetes medication etc., their costs would go down. The plans are controversial but there is at least some evidence that they work. In the long run this should improve the health of plan members and reduce health care spending over time. For example Safeway reported:
“…the proportion of employees classified as obese declined by five percentage points, while the proportion who were overweight declined by one percentage point. Meanwhile, 40 percent of workers and spouses who failed the blood pressure test in 2008 passed in 2009, 30 percent of former smokers registered as tobacco-free, and 17 percent who failed the cholesterol test in 2008 passed in 2009.”
Absent in the discussion is rating people based on their physical fitness. As an exercise advocate this makes sense to me because exercise is a powerful modifier of other health risk factors.
My take is that a large fraction (estimates are in the 60-90% range) of our health and the diseases we get have major behavioral components. We also know that only a limited number of people follow key health guidelines and practice what might be described as personalized preventive medicine. Should those of us who do follow the guidelines subsidize insurance premiums for those who don’t? That having been said, I think insurance plans that reward personal responsibility are essential to improve public health and reduce health care expenditures –a potential win-win for us all. Premiums schemes that encourage personal responsibility are probably only one part of a comprehensive plan to address lifestyle related diseases, but it seems to me the more messages we send people about the importance of personal responsibility for their own health the better.
Aging: Just the Facts
A couple of posts ago I showed you a pie chart of what the US Federal Government spends money on and more than 50% of the total goes to Social Security and Medicare — people who are mostly over 65. This means that our aging population is driving much of the pressure on the budget and will be central to the debate about spending and taxes that continues now that the election is over. That having been said, I think it is essential for us all to have some appreciation of why aging is going to be such a big challenge. The chart below comes from something on the history of Social Security and shows how many people made it to 65 and how long they lived on average after they made it to 65. It starts in 1940 and ends in 1990.
| Percentage of Population Surviving from Age 21 to Age 65 | Average Remaining Life Expectancy for Those Surviving to Age 65 | |||
| Male | Female | Male | Female | |
| 1940 1950 1960 1970 1980 1990 |
53.9 56.2 60.1 63.7 67.8 72.3 |
60.6 65.5 71.3 76.9 80.9 83.6 |
12.7 13.1 13.2 13.8 14.6 15.3 |
14.7 16.2 17.4 18.6 19.1 19.6 |
When you update the data in this chart for 2010, it turns out that about 84% of men and 89% of women now make it to 65. The next figure shows that people live even longer now after they make it to 65. The average man who makes it to 65 lives another 16-17 years and for women it is about 19 years. These numbers are projected to continue to rise for both sexes.

When you put all of this together there is going to be a huge increase in the number of people over age 65 as the Baby Boom generation of roughly 80 million people born between 1946-64 ages. The number of people over age 85 is also going to grow rapidly. The figure below shows those numbers.

I would argue that however we as society ultimately decide to deal with the budgetary challenges ahead via our chaotic political process, we need to do it in a way that fully accounts for the fact that almost all of us will live to be 65 and many of us will make it to 85 or older. I am sure there are people reading this who think we should raise taxes and/or spend less on defense to preserve Social Security and Medicare as they are, others who think benefits should be scaled back, others who think things should be privatized, and others who might do some of all of the above. However, if we are going to do things that both make sense and are politically possible I think we first need a serious dose of demographic reality injected into the discussion. I hope you find the data above useful.
Aging & the Post Election Medicare Debate
In my post just before the election I covered some ideas about what was missing and also some of the inconsistencies in the politics of health care. I also described some of the main factors driving the rise in health care spending including an aging population.
In the next few months both parties will face the so called “Fiscal Cliff” which consists of the expiration of the Bush era tax cuts (e.g. tax increases) and automatic spending cuts that were put in place in 2011. At some level this represents mutual political blackmail by both parties. The thinking goes that the Republicans don’t want the tax increases or cuts in defense spending and the Democrats don’t want cuts in other programs. Thus both parties might actually be incented to reach some sort of compromise and put the long term fiscal health of the country on the right track reminiscent of what Ronald Reagan and Tip O’Neill in the 1980s when they fixed Social Security. If a compromise does emerge, changes in Medicare and Social Security are going to be big topics of the discussion and solution.
I want to show two graphics that I hope will help everyone understand the magnitude of the problem and inform their own thinking about it.
First, both taxes and spending are part of the problem. The figure below is from an excellent pre-election Wall Street Journal article on trends in taxes and spending. It shows that the big yearly deficits recently being run in the U.S. are due to a combination of low taxes and high spending by recent standards.

Second, here is a figure of where the Feds spend money as exemplified by the proposed budget for 2013 (it has not been passed yet). The total is just under $3.7 trillion. What is interesting is that a total of 62% is “mandatory” spending on things like Social Security and Medicare. Another 18% or about $65O billion is for the military, and interest on the debt is 7%. With current policies in place the deficit is expected to be about $1 trillion. So even if you cut everything else (Ag programs, medical research, education etc.) to zero you would still have to raise taxes by about $500 billion per year to balance the budget and pay for mandatory programs, the military and interest on the debt. The other long term issue is that most of the mandatory spending is tied to Social Security and Medicare that are for people over 65. Thus these programs are set to grow automatically as the baby boom generation ages and there are more people over 65.

The next link is to a budget calculator game from 2010 that lets you figure out what combination of spending cuts and changes in tax policy you would consider to address the long term budget issues facing the country. I would encourage everyone to play the budget game, we all need to educate ourselves about these issues and understand the choices we face. The goal of the graphics above and the budget game is to give readers the resources to learn more. The simple math I have outlined suggests that changes in Social Security and Medicare spending are coming. More on this in upcoming posts.
Health Care and the Election
Tomorrow is the long awaited election. What strikes me is that most of the discussion about health care has been about the pros and cons of various flavors of what might broadly be called “insurance reform”. Who should be covered? What should be covered? How do we pay for it? How is it regulated? What is the balance between the private sector and government be? Central to all of these concerns are a few big issues:
- In the U.S. we spend a huge fraction (almost 18%) of our GDP on healthcare and yet our public health statistics are not particularly impressive.
- The rise in spending on healthcare in general and Medicare in specific is not sustainable.
- There is a lot of unnecessary spending on procedures and tests – overuse of technology – that probably don’t improve patient outcomes.
- There are a lot of uninsured people, and there is also a lot of political gridlock.
These are all interesting facts, but to me the current political arguments are mostly missing the bus.
Spending vs Public Health Statistics.
The determinants of population health don’t have much to do with the formal healthcare (sick care?) system. I have seen estimates suggesting that 60-80% of population health is about lifestyle, culture and behavioral choices. So, we need to stop confusing what happens when “people go to the Dr.” with public health statistics. As I have pointed out in areas like smoking and traffic safety the U.S. has an excellent track record and many of these strategies could be applied to obesity and inactivity. Also is it fair to compare the U.S. as a whole to smaller more homogenous countries in Europe. When you match various U.S. states with specific countries, things look different. Things are not the same in Athens as they are in Oslo, why should they be the same in Miami and Minneapolis?
Medicare Spending.
I have just a couple of comments on the rise in Medicare spending. At some level doesn’t this represent the problem of “success”? Every developed country in the world and most of the developing countries in the world are undergoing huge shifts in population structure. Humans as a whole are living longer and in 2000, for the first time in world history, there were more people over 60 than under 5. That having been said, I would argue that no matter what we do in terms of “insurance reform” for Medicare in the U.S., it is going to be too little too late in terms of finances unless we promote healthy aging. So again is the problem simply money and resources; or is it really a matter of lifestyle, culture and behavior? There was an interesting article in the NYT magazine on an Island in Greece with a whole bunch of healthy older people, and the story of these islanders is essentially the same old story for healthy aging. Don’t smoke, be active, don’t get fat, stay socially engaged etc.
Overuse of Technology.
The best estimates are that the overuse rate for most things in medicine is about 30%. The question then is how do you turn this around? Some argue that more regulation is needed; some argue that electronic medical records will fix it; some argue that the market can fix it. My guess is that depending on the specifics it will be some of the above, all of the above and none of the above at the same time. However, why not avoid the need for costly interventions by focusing on the root causes of what drive medical costs in the first place? I have said it before, the root causes of what ails us are embedded in our lifestyle, culture and behavior. Why not focus on these issues?
The Uninsured vs. Political Gridlock.
Among the many things I find ironic about the political debate on healthcare reform is the fact that the individual mandate in Obamacare was originally developed by conservative thinkers. Along similar lines ideas about premium support now championed by Paul Ryan (e.g. vouchers) were initially developed by liberal policy wonks. Go figure? How will we ever address the issues of the uninsured, costs, overuse of technology, obesity, inactivity, aging and everything else associated with healthcare if policy ideas are merely ropes in an ongoing political tug of war?
Is there a solution?
I think in the short and medium run we should all do two things:
- Take responsibility for our own health by following key guidelines that I have discussed over and over again in my posts.
- Indicate to the political leadership that focusing on public health initiatives might be a good (and cheap) first step they could all agree on.
If we all did these two things maybe that would give them some time to learn that thoughtful compromise on the other issues will not be fatal and pragmatism is not a disease. Denial can be both.
You are currently browsing the archives for the Health Policy category.
LIKE MIKE

SUBSCRIBE TO RSS
