
Archive for March, 2015
Too Much, Too Much Exercise?
There has been yet another wave of “too much” exercise stories in the media based on a recent study of 1 million women from the UK. The idea is that moderate levels of physical activity most days with occasional bouts of strenuous activity can cause big drops in both cardiovascular and all-cause mortality. However, doing a lot of hard training is not as beneficial.
This topic has been recycling for the last couple of years. Alex Hutchinson (who has a Ph.D. in physics) has done an excellent numerical/statistical breakdown on one of the key studies that “supports” the too much exercise hypothesis. Put simply there are many limitations to the whole argument. I have done a couple of posts on what both the epidemiology and physiology tell us on the topic. The first was in 2012 and another one with Brad Stulberg in 2014. I too am a skeptic.
I am in the camp that 30-60 minutes of physical activity most days is the sweet spot for general health and that more is not better, but it is not worse either. Those who really push it most days are also likely motivated by things other than return on investment thinking about their health. Perhaps they want to compete in races or are into pushing themselves to meet more hard core physical goals.
The Swedish Skiers
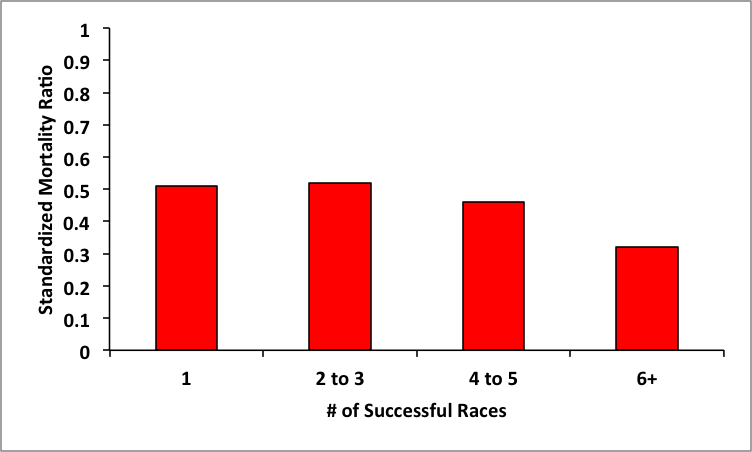
Whenever this topic comes up I also bring up a paper that followed about 50,000 male finishers of the 90km (~55 miles) Vasaloppet cross country ski race in Sweden. This study used the Swedish medical records system to look at mortality in the race finishers. In preparing for an upcoming talk on exercise and health, I asked my colleague Andy Miller to generate some figures from the skiing study. The one below shows that mortality is about 50% or less than predicted for race finishers compared to the expected rate gleaned from Swedish population records. It also shows that finishing more races was not associated with an uptick in mortality, if anything it was associated with a down tick. Who knows exactly what these folks were doing, but those who finished a number of races certainly had to be doing a lot of strenuous training over many years.
Summary
I have repeatedly asked those in the “too much” much camp to rebut this paper and point out any major flaws in it. The bottom line is that it is at least as strong or stronger than the studies “supporting” the too much exercise hypothesis. Until data comes along that clearly refutes the data in the chart above I will remain a skeptic.

Identical Twins & Genetic Destiny
There is a fascinating recent study from Finland on pairs of identical twins with very different exercise habits. This is unusual because widely divergent behavior patterns between identical twins are uncommon. There were some pretty striking differences in thinks like exercise capacity, metabolism and even brain structure in the active vs. inactive twins showing that even when the “genes are the same” behavior can really make a difference. The details of the paper were beautifully summarized by Gretchen Reynolds in the New York Times with some excellent insights from the authors of the paper included in her article. Some additional thoughts about what this all means are available in an excellent commentary by Alex Hutchinson in Runner’s World.
This study and the outstanding pieces by Gretchen and Alex reminded me of a paper from the early 1980s on the different physiological adaptations to strength and endurance training. The paper included the pictures below of identical twin brothers. One was an endurance runner, the other a weight lifter.
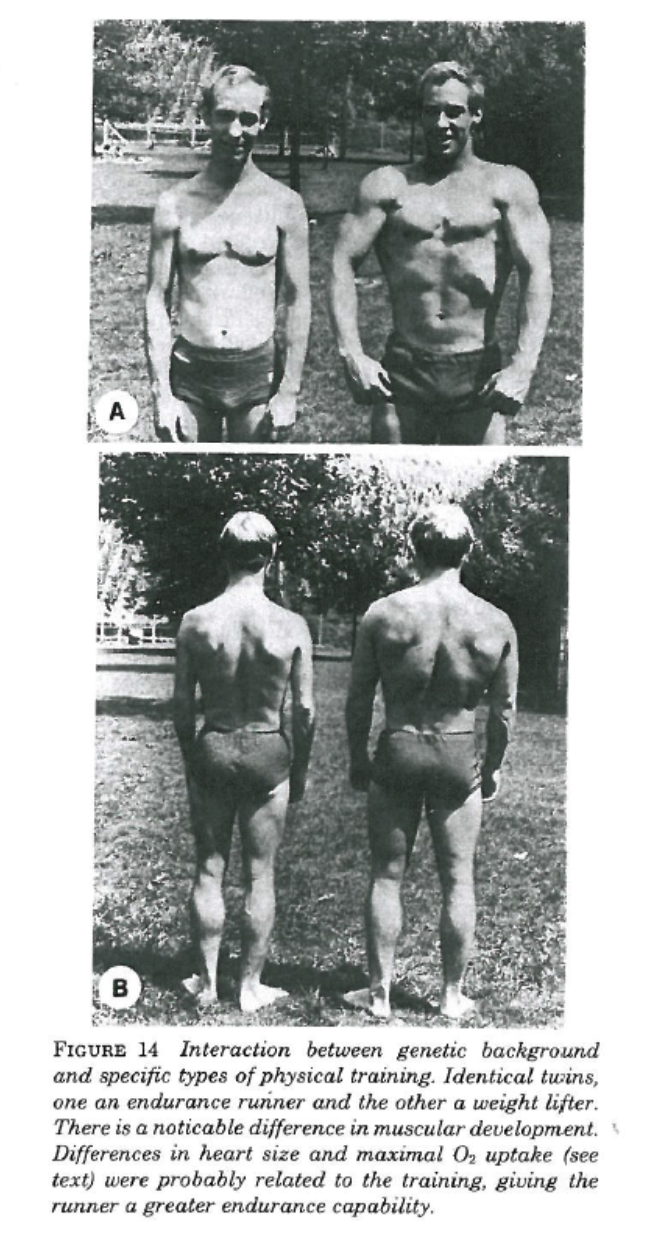
The picture speaks for itself. The lifter was 16kg (35 lbs) heavier than the runner, but the runner’s heart was about 25% larger and his maximal oxygen uptake more than 50% greater than his brother’s. Of note, the height of the brothers and things like their hair patterns are strikingly similar. For those who want to know more about the strengths and limitations of twin studies and what can be inferred from them here is an informative link.
That such big differences in physiology can be seen in people who have “identical” genes is pretty convincing evidence that for many things our genes are not our destiny.
Precision Medicine & Precision Weather: A False Analogy?
One of the ideas riding the wave of enthusiasm for precision medicine is that with enough big data it should be possible to make increasingly accurate “forecasts” about who gets what disease and how it might be prevented, treated or even “cured”. An analogy to precision weather forecasting and climatology is frequently drawn. Cynicism aside about just how good weather forecasting is and how much it has improved, there are a couple of basic intellectual issues with the comparison that are typically glossed over by advocates of the analogy.
Problem 1: The Nature of the Data
Weather data includes things like continuously monitored surface temperature and wind patterns over essentially most of the world. Some of the data is very granular with high spatial and temporal resolution. Things like pressure measurements, above ground temperatures, below ground temperatures, satellite photos, and information on things like humidity are available. There is also a vast store of historical records dating back 100 or more years in many places. This type of multilevel, highly accurate data with essentially continuous time resolution is simply not available even in the most monitored humans living in the real world even with the best monitors. The accuracy of various wearable devices, the granularity of the data, and the historical information they provide pales in comparison to the available weather related data. As someone who has been making some the most detailed possible measurements of human physiology since the late 1970s, things have been miniaturized and made portable, but the quality of the data has not improved and in many ways has gotten sloppier or at least harder to calibrate.
Problem 2: Predicting What?
The other thing to remember is that with weather prediction the goal is to predict what it is going to be like “outside” in a given place on a given day at a given time. Precision weather forecasting does not tell us anything about the temperature and humidity inside “your house” much less inside a given room inside the house. To make that sort of estimate all sorts of additional information is needed about the size of the house, the surface area exposed to the outside world, the heating and cooling system, how insulated the house is, how good the thermostat is etc., etc, etc… Then there is always the possibility that a window is open or that on a cold day you choose to wear a sweater and reduce the temperature “set-point” on the thermostat. The same issues also apply to a given room the house.
The point here is that for human disease, except perhaps for some elements of dermatology, we are generally interested in what is happening inside a specific room inside the body like the “heart” room, or the “liver” room or the “kidney” room. For things like diabetes or high blood pressure that affect multiple rooms, we are interested in the overall house. Also many diseases of specific rooms also frequently do collateral damage to “the rest of the house”. In many of these diseases the ultimate problem that “brings people to the Dr.” has something to do with a complex feedback control system that has gone haywire. That is certainly the case for diabetes, heart failure, and high blood pressure. In heart failure shortness of breath and exercise intolerance is usually the problem patients complain about vs. a weak heart.
So the weather is an outside condition we are trying to predict based on outside data. Medical conditions are generally inside conditions and predicting them from outside data of questionable quality with limited time resolution and historical tracking is clearly an area where the precision medicine vs. precision weather analogy breaks down. Things like biopsies, images and blood tests are inside samples but they are small snap shots and not the sort of continuous measures available to the weather forecasters
Even if we had perfect monitors it remains to be seen if people will actually use them and if the information gained does anything to change their behavior or make them healthier.
Problem 3: What About Inside-out Prediction?
The flip side of the weather analogy is the idea that if you know enough about the building blocks (the cells for example) that make up the house you can predict what is going on inside the house as a whole. Of course the outside world influences what is happening inside and those who favor an inside-out paradigm tend to ignore or discount that problem. Another issue is that unlike static structures humans can move around and change their behavior depending on the conditions outside. When I lived in Arizona I went outside mostly during the cooler parts of the day. In Minnesota where I now live, most of the year, I go outside during the warmer parts of the day. A cell based approach to modeling what is going on inside the body can miss this key but obvious point.
Then there is the problem of the cells as building materials. Imagine decorative concrete blocks like the ones used in the wall shown below.
Depending on the orientation of such blocks, a wall made from them can have very different properties. Flip them on their side and a solid vs. porous wall “emerges”. Thus, the temperature inside a structure made from such concrete blocks could vary widely depending on their orientation. However, subject the blocks from a wall of any design to chemical analysis and the “basic” properties of the wall are the same. Things of course get even more complicated if you add a heating and cooling system with a thermostat or other design features that influence the temperature in your concrete block building. This sort of inside-out modeling would be less problematic if the DNA in our cells was a better blueprint for what the “whole building”, but it turns out that DNA is a pretty sloppy and much more adaptive blue print than was once thought.
Closing Comment
I would be curious to see just how much better or accurate weather forecasting has gotten over the years. If there is data on this topic perhaps someone will post a source in the comments section. In the meantime, I hope the concepts noted above make you question the precision medicine, precision weather analogy.
Fitness & Mortality Update
Two recent scientific papers make it time for a quick update on the topic of fitness and mortality.
1. Fitness vs. Cancer Mortality
The first paper is meta-analysis that summarizes the results of a number of studies on the relationship between fitness and cancer mortality. The results were pretty striking:
“Six prospective studies with an overall number of 71 654 individuals and 2002 cases of total cancer mortality were included. The median follow-up time in the studies was 16.4 years. Cardiorespiratory fitness showed a strong, graded, inverse association with total cancer mortality. Using low cardiorespiratory fitness as the reference group, intermediate and high levels of cardiorespiratory fitness were related to statistically significant decreased summary relative risks (RRs) of total cancer mortality of 0.80 [95% confidence interval (CI) 0.67-0.97] and 0.55 (95% CI 0.47-0.65), respectively. Studies that adjusted for adiposity yielded similar results to those that did not adjust for adiposity.”
This means that folks with high cardiorespiratory fitness have about half the risk of death from cancer as people in the low fit group. Usually, in these types of population studies “high fit” is defined as the ability to do “10 mets” of exercise. For example a person with a 10 met exercise capacity can typically run 6 miles (10 km) per hour for few minutes at the end of a maximum exercise test. This is also an exercise capacity that many if not most middle aged people can attain if they watch their weight and workout regularly. So while physical activity and cardiorespiratory fitness are not the same thing, many active middle aged people can get to 10 mets. The flip side of this relationship is that most highly fit people are also pretty active and they do at least some higher intensity exercise training which makes it likely they have a 10 met exercise capacity.
2. Fitness vs. Cardiovascular mortality
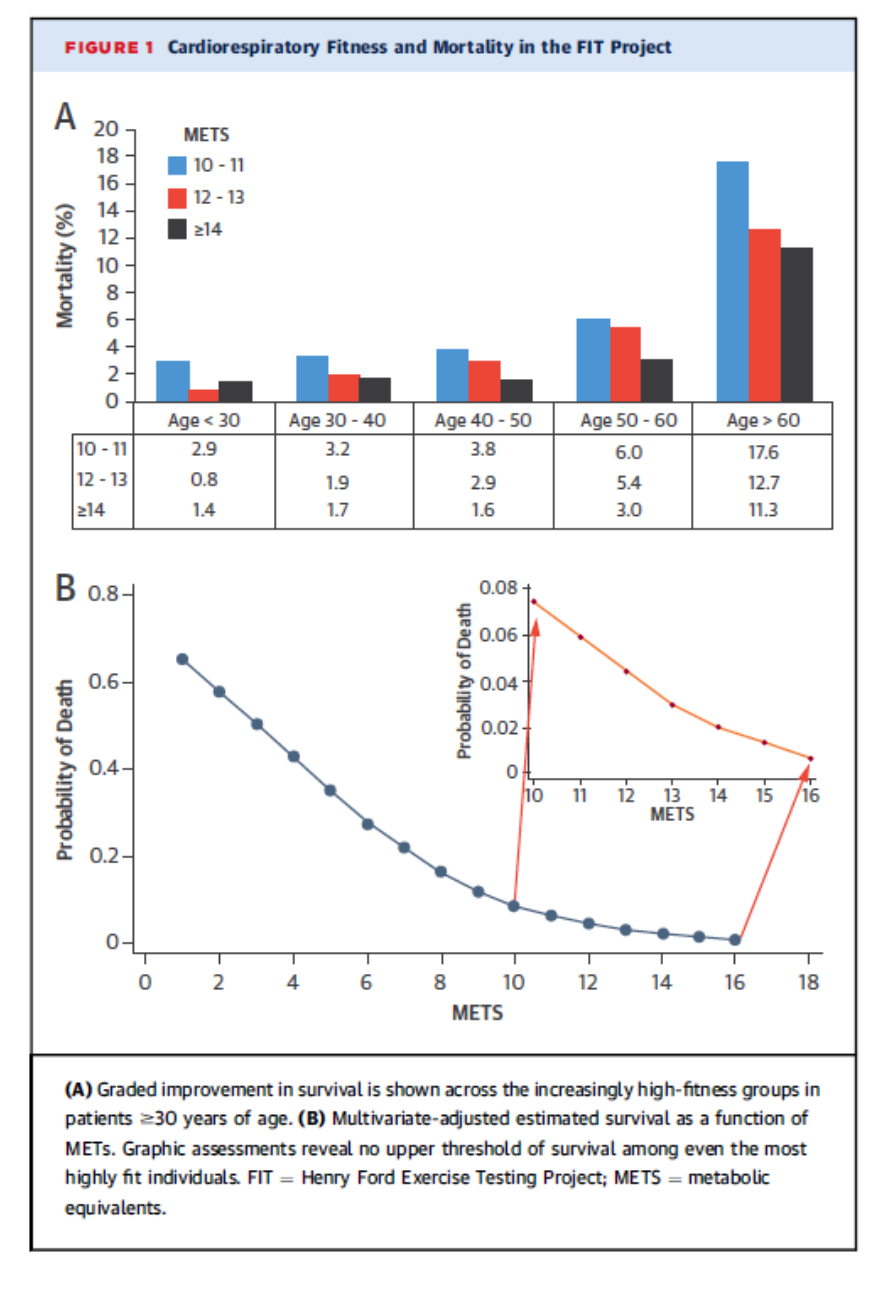
It has been known for a long time that increased fitness is associated with both lower all-cause mortality and lower cardiovascular mortality. A remaining question is whether this relationship flattens out at about 10 mets. In other words do people who can do more than 10 mets have even lower mortality? The graph below comes from a short report on this topic in almost 70,000 people (64% men) followed for about 12 years including about 38,000 with an exercise capacity of greater than 10 mets. The top panel shows that very high fitness was associated with lower mortality in all age groups. The bottom panel shows the dose response relationships between fitness for the entire study population. So greater fitness equals lower mortality.
Summary
Evidence for the protective effects of fitness and its close relative physical activity keeps piling up. The cancer data is especially heartening, and that fact that things don’t flatten out for fitness vs. mortality at very high levels of fitness is perhaps another piece of objective evidence against the too much exercise “hypothesis”.
You are currently browsing the Human Limits blog archives for March, 2015.
LIKE MIKE

SUBSCRIBE TO RSS
